

Summary Card
Definition of Intrinsic Plus
Intrinsic Plus condition is marked by tight interossei and lumbricals muscles causing MCPJ hyperflexion and PIPJ hyperextension, initially identified by Finochietto in 1920 and elaborated by Bunnell in 1946.
Intrinsic Muscle Anatomy
Interossei and lumbricals contribute to MCPJ flexion, IPJ extension, grip, and pinch strength in hands.
Intrinsic Plus Aetiology
Intrinsic tightness can stem from local issues like fractures or systemic conditions like Rheumatoid Arthritis, affecting the interosseous muscles.
Intrinsic Plus Clinical Picture
Diagnosis involves identifying reduced PIPJ flexion in MCPJ extension (Bunnell's Test), with severe cases leading to non-correctible contractures and swan-neck deformities.
Non-Surgical Management of the Intrinsic Plus Hand
Non-surgical treatment aims to prevent irreversible contractures, employing methods like elevation, splinting, and manual stretching depending on the joints involved.
Surgical Management of the Intrinsic Plus Hand
Surgical options vary based on severity and affected joint, ranging from distal/proximal releases to muscle slides or ulnar neurectomy, targeting the restoration of hand function and correction of deformities.
Definition of Intrinsic Plus
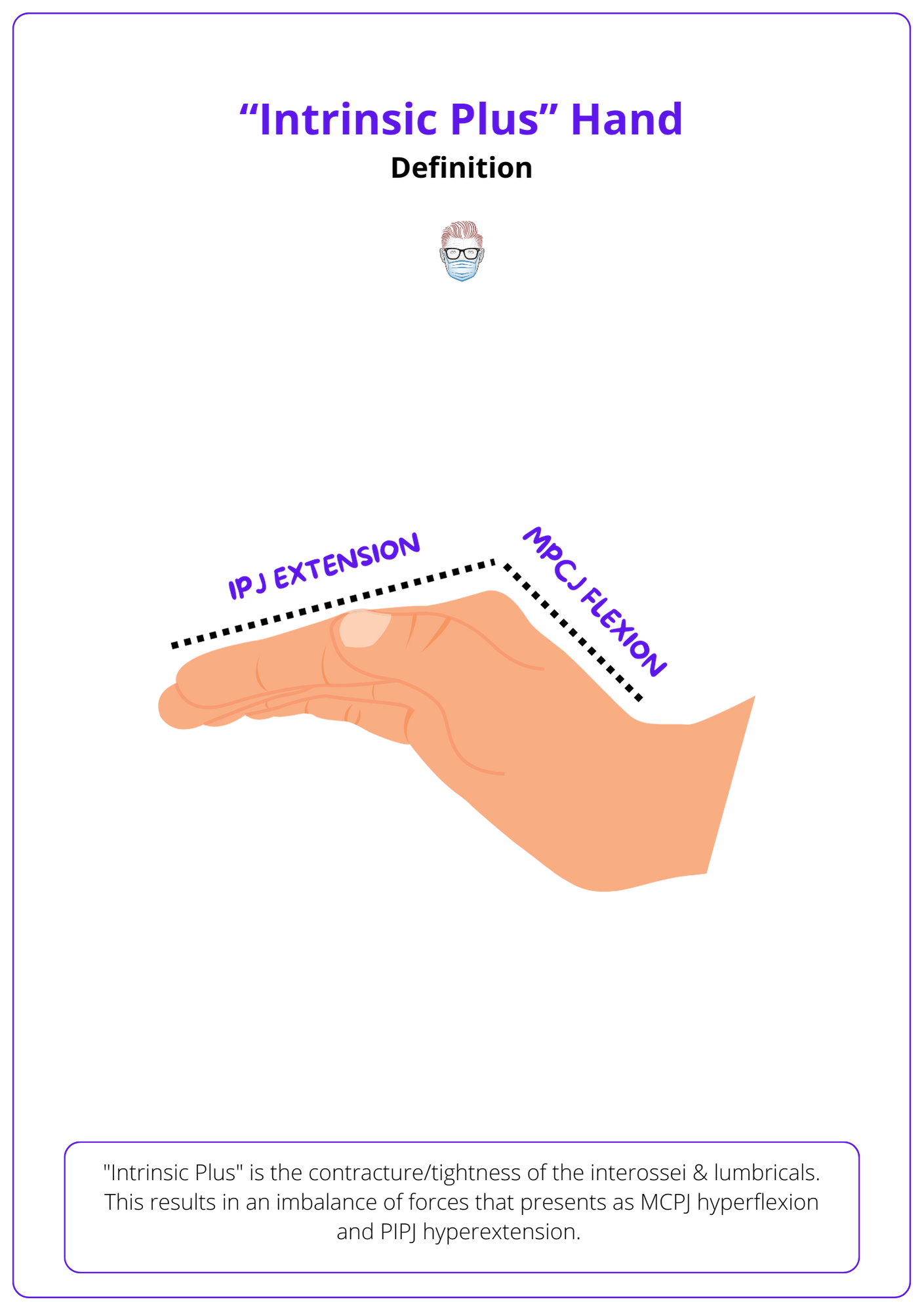
"Intrinsic Plus" is the tightness of interossei & lumbricals causing MCPJ hyperflexion and PIPJ hyperextension, first noted by Finochietto in 1920 and detailed by Bunnell in 1946.
"Intrinsic Plus" is the tightness of the interossei & lumbricals. This results in an imbalance of forces that presents as MCPJ hyperflexion and PIPJ hyperextension. Chronic tightness can result in contractures and swan-neck deformities.
It was described by (Finochietto, 1920) and later expanded upon by (Bunnell, 1946).
Intrinsic Muscle Anatomy
Interossei and lumbricals muscles provide MCPJ flexion and IPJ extension. They also contribute to grip strength and pinch strength.
An intrinsic muscle is defined as those having an origin and insertion within the hand. This includes the thenar and hypothenar muscles, interossei, and lumbricals. In general, the fingers are controlled by 6 muscles
- 3 intrinsic: dorsal and palmar interossei, lumbrical
- 3 extrinsic: FDS, FDP and EDC (index & little have an extra extensor)
The intrinsic muscles produce MCPJ flexion and IPJ extension because the muscles travel volar to the axis of rotation of the MCPJ but dorsal to the axis of rotation of the IPJ.
Interossei
The fingers are stabilised by 4 dorsal & 3 volar interossei. These muscles' primary functions are:
- MCP flexion/stabilization and IPJ extension.
- Palmar interossei also adduct the finger
- Dorsal interossei also abduct the finger (Lauer, 1999)
Please note that the little finger has a slight variation in horizontal movements. The little finger is abducted by the extensor digiti quinti and abductor digiti quinti. Below is the visualization of this.
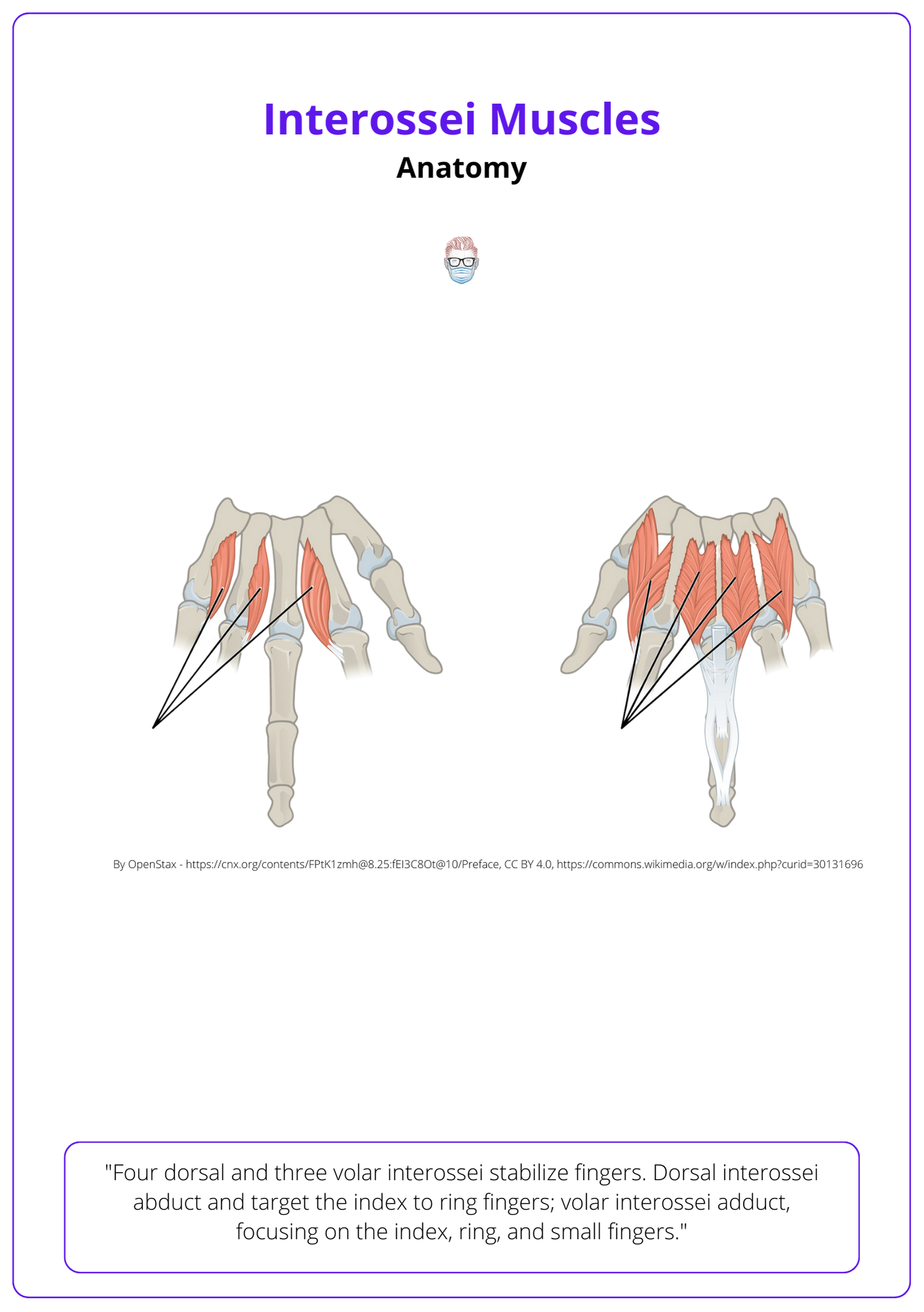
These muscles originate on the side of the metacarpals. Their insertion points differ. Volar interossei insert onto the index, ring, and small fingers. Whereas the dorsal interossei insert onto the index, middle and ring. More specifically:
- 1st interosseous inserts onto the index finger.
- 2nd and 3rd interossei insert onto the middle finger
- 4th interosseous inserts onto the ring finger.
The action of these muscles largely hinges on their insertion sites, not their origin. Therefore, they have often been classified based on their insertion site (Stack, 1962 and Zancolli, 1979)
Lumbricals
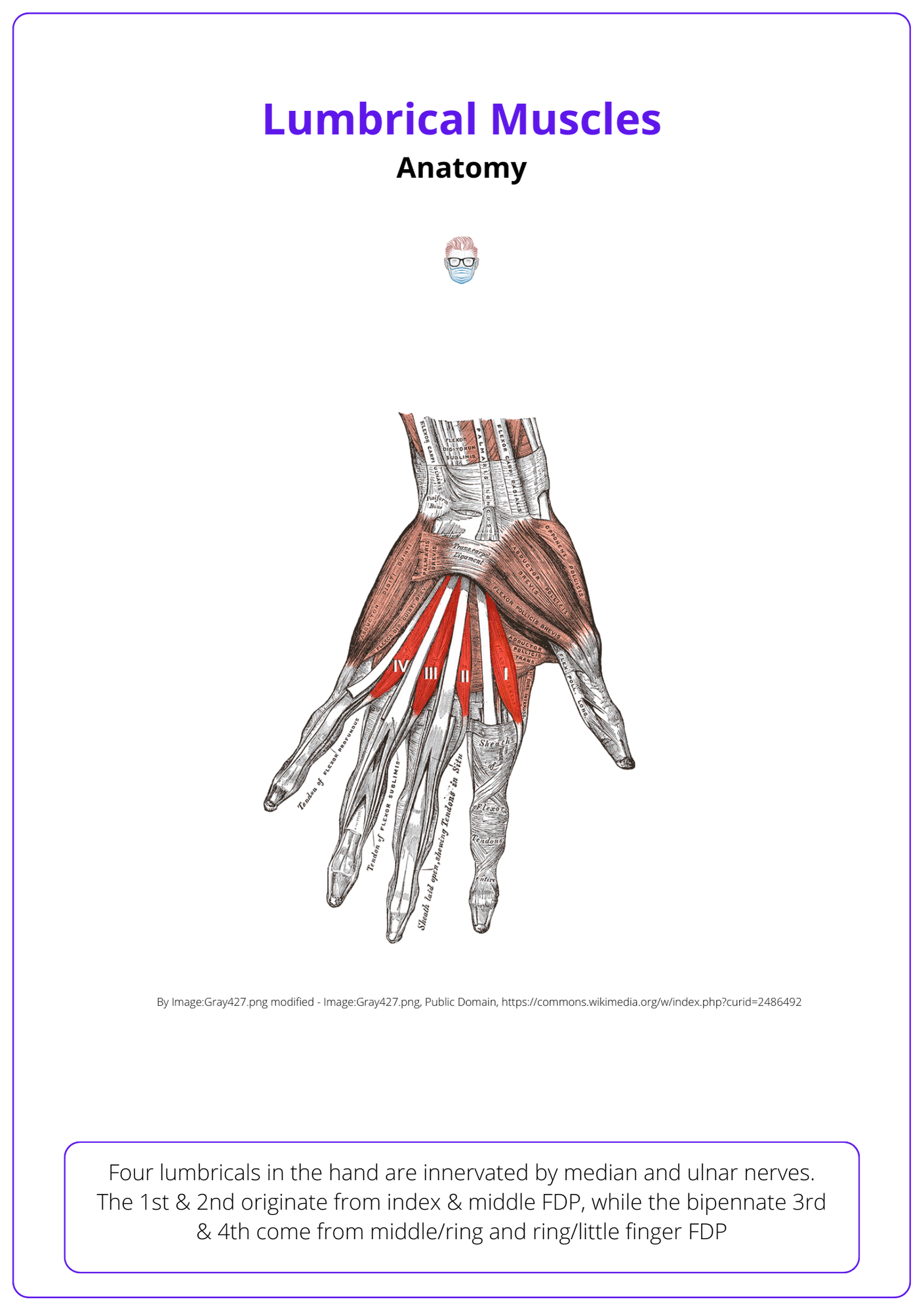
There are 4 lumbricals in the hand innervated by the median (radial lumbricals) and ulnar (ulnar lumbricals) nerves.
- 1st & 2nd lumbricals originate from the radial side of index & middle FDP, insert onto the dorsal expansion as the radial lateral band.
- 3rd & 4th lumbricals are bipennate & originate from the middle/ring and ring/little finger FDP.
Here is the anatomy of the lumbrical muscles.
Intrinsic Plus Aetiology
Intrinsic tightness, shortening of interosseous muscles, arises from local issues (e.g., fractures) or systemic conditions (e.g., Rheumatoid Arthritis).
Overview
Intrinsic tightness/contracture is the shortening of the interosseous muscles. It can be the result of ischaemia, adhesions, displacement, or spasticity. These pathophysiological states are associated with localised or systemic conditions:
- Localised: fractures, infection, burns, compartment syndrome, lumbrical-plus
- Systemic: Rheumatoid Arthritis, spasticity
Fractures
- Metacarpal fractures can result in oedema, immobilization, adhesions and ultimately fibrosis of the tendons and muscle bellies (Paksima, 2012)
- Proximal phalanx fractures can displace the lateral bands and stretch with callous formation. Adhesions may also form within the lateral bands, which would reduce PIP flexion regardless of MCPJ position (Paksima, 2012). This is why some extra-articular proximal phalanx fractures can still affect the PIPJ movement post-operatively.
Mallet finger
- Redirects intrinsic force solely to the PIP joint
- Can progress to swan neck deformity and intensifying intrinsic contracture due to volar plate attrition (Schweitzer, 2004).
Lumbrical Plus Finger
- Cause: FDP injury distal to the origin of lumbrical, lax tendon graft, distal amputation, high median nerve palsy.
- Effect: FDP (lumbrical origin) retracts proximally, increases tension on the lumbrical & its insertion (lateral band) (Parkes, 1971)
- Result: "paradoxical extension" of the PIPJ with flexion/difficult PIPJ flexion.
Rheumatoid Arthritis
- These intrinsic tightness types result from adhesions, inflammation & potentially hypoxia (Akhavani, 2011).
- Rheumatoid arthritis can also cause intrinsic contractures due to MCPJ dislocations and ulnar deviation (Heywood, 1979)
Spasticity
- This can be related to cerebral palsy, stroke, tetraplegia, or traumatic brain injuries. It can be associated with shoulder & elbow contractures.
Intrinsic Plus Clinical Picture
"Intrinsic plus" hand is clinically diagnosed through reduced PIPJ flexion in MPCJ extension (Bunnel's Test). Severe cases can cause non-correctible contractures and swan-neck deformities.
An "intrinsic plus" hand is a clinical diagnosis that can be supported by specific investigations to identify the aetiology. It is important to note that intrinsic tightness describes a less severe process - PIPJ flexion deficiency is still passively correctable.
Loss of grip strength
Patients may complain of difficulty with grasping large cylindrical objects. This is because of a restricted PIPJ when the MCP is extended. More specifically:
- Normal Intrinsics: when the fingers grasp around a large sphere, the FDP, FDS and intrinsic simultaneously flex the DIPJ, PIPJ and MCPJ, respectively
- Abnormal Intrinsics: IPJs flex before the MCPJs to produce a hook fist. There is also limited PIPJ flexion when MCPJ is extended.
Patients are often still able to flex the IP joints due to the flexor tendons ability to overpower the intrinsic.
Bunnel's Test
The intrinsic tightness test was developed by Bunnell in 1946.
- Step 1: passively extend MCPJ (stretch intrinsics), measure PIPJ flexion.
- Step 2: passively flex the MCPJ (relaxes intrinsics) and measure PIPJ flexion
- Result: a PIPJ flexion increase suggests isolated intrinsic tightness.
Below image visualizes the Bunnell Test.

This test can be also performed in radial or ulnar deviation. For example, placing the MCPJ into radial deviation during the test would further tighten the ulnar-side intrinsic tendons.
Swan neck deformity
A swan neck deformity can occur in severe chronic contractures by the following mechanism.
- Cause: Progressive PIPJ contracture leads to hyperextension.
- Effect: Terminal tendon slackens while the FDP tendon tightens.
- Result: DIPJ flexion ensues, leading to a swan neck deformity. Over time this can result in volar plate attenuation or collateral ligament capsular contraction
Here's a visual representation of Swan Neck Deformity.

Investigations
An intrinsic-plus hand is primarily a clinical diagnosis. Adjunctive investigations can be considered, such as:
- Isolated strength & pinch measurements.
- X-rays to assess subluxation in rheumatoid patients.
- Rheumatoid serology testing.
- Nerve block in spasticity before the intrinsic tightness test can assist the examiner in discerning increased muscle tone from fixed contractures.
- Dynamic electromyography (EMG) to evaluate the level of volitional control.
Non-Surgical Management of the Intrinsic Plus Hand
Treatment for finger intrinsic contractures depends on the cause. Determine whether it involves just the PIPJ or both PIPJ and MCPJ to guide management.
The primary goal of treatment is to prevent a contracture that is no longer passively correctable. Non-surgical treatment should be continued until progress is no longer observed. Options include:
- Elevation to reduce oedema, serum protein deposition and scar tissue formation.
- Splinting in the intrinsic plus position (MCPJ flexion 70°, IPJs in extension) to optimise the MCPJ collateral ligaments & keeps intrinsics in a shortened position.
- Manual stretching of the intrinsics by passive abduction or by MCPJ extension and IPJ flexion (Seu, 2012).
- Progressive static splints hold the MCP joints in extension and allow passive hook exercises (ie: perform the intrinsic tightness test).
Surgical Management of the Intrinsic Plus Hand
Mild intrinsic tightness can be treated with hand therapy or distal release. Severe disease requires correction of swan neck deformity. Nonfunctioning intrinsics may be completely released or denervated.
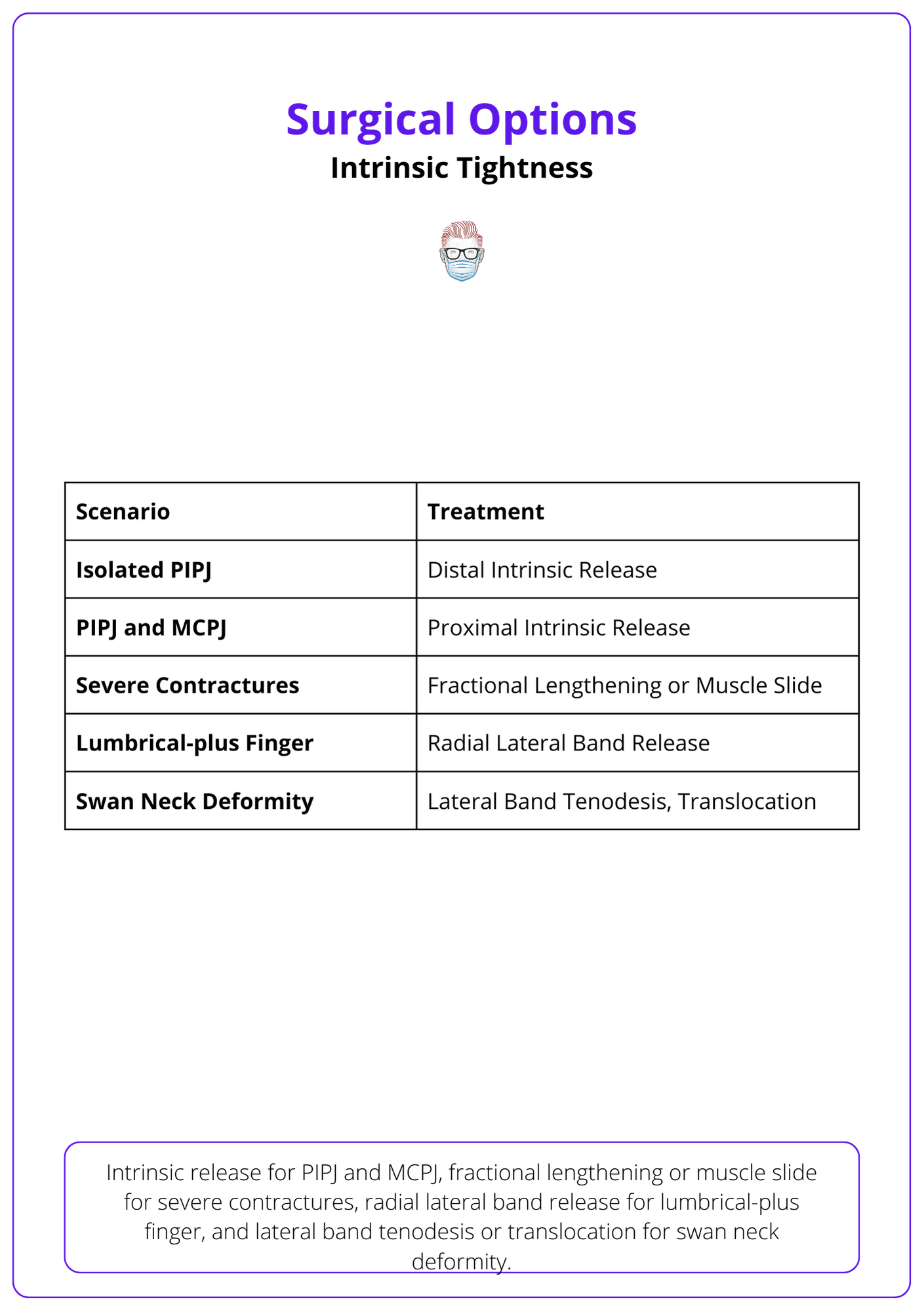
A variety of procedures are available to the intrinsic-plus patient. The choice is dependent on the aetiology, severity and most importantly the joint involved. Options include proximal and distal releases, slides, or translocations.
Below table shows the surgical treatment options available for Intrinsic Tightness.
PIPJ Treatment
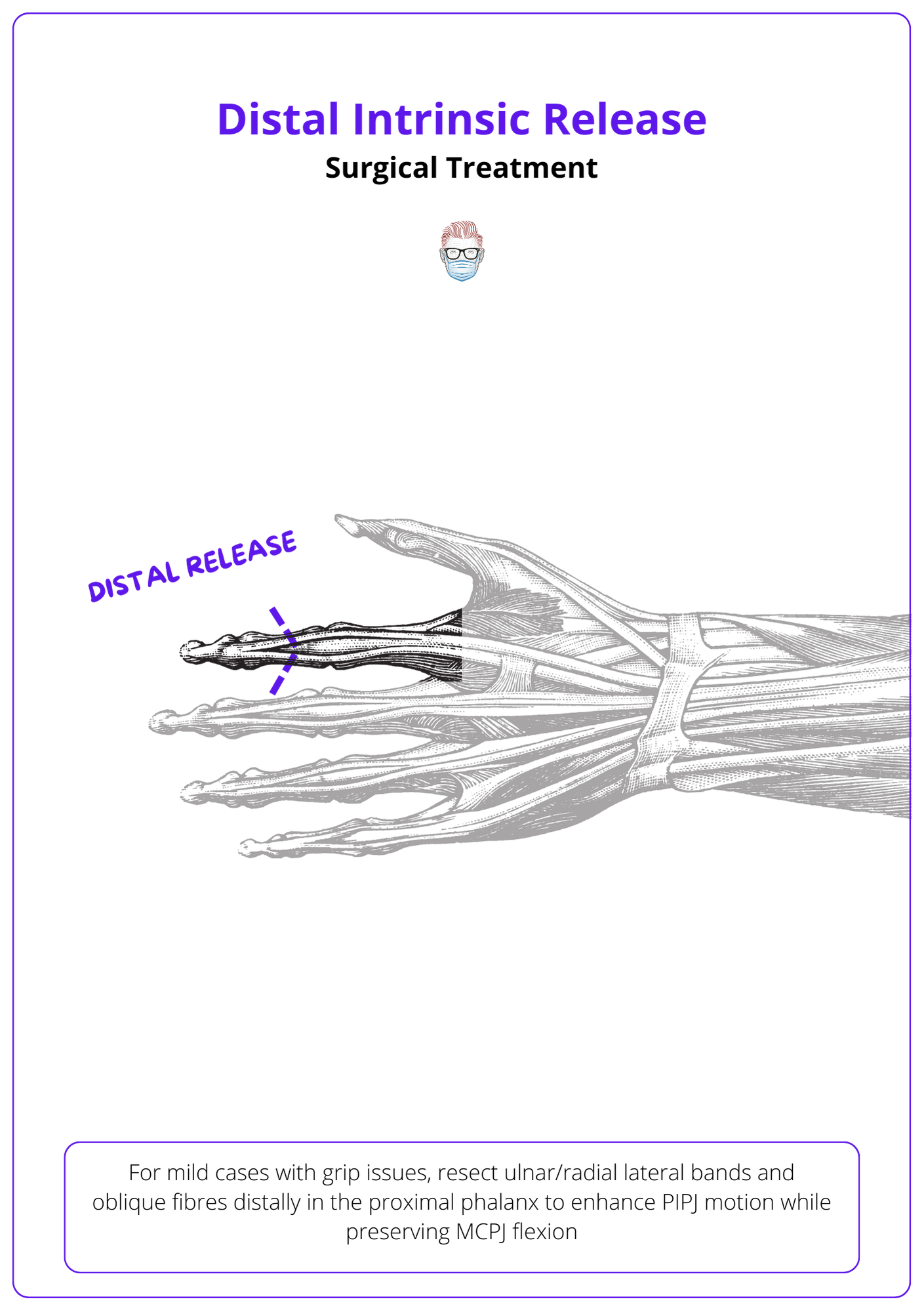
Distal Intrinsic Release for PIPJ
- Indication: Consider mild cases to improve PIPJ motion when patients struggle to make a full fist or weakness of grip.
- Purpose: decrease the intrinsic force on the PIPJ without affecting the intrinsic flexion of the MCPJ.
- Technique: resection of the ulnar and/or radial lateral bands & oblique fibres in the distal third of the proximal phalanx. This is distal to the transverse fibres that are responsible for MCPJ flexion. If the release is inadequate, then progressively more volar and proximal tissue is released until passive PIPJ flexion is achieved. (Espiritu, 2011)
Here is a visual representation of Distal Intrinsic Release.
MCPJ Flexion Treatment
MCP flexion contractures secondary to intrinsic tightness are treated based on severity and aetiology. Options include a proximal intrinsic release (PIR), intrinsic muscle slide, botox injections, or ulnar nerve neurectomy.
Proximal Intrinsic Release
- Indication: MCPJ flexion contracture when intrinsic muscles have become fibrotic and no intrinsic muscle function is anticipated:
- Technique: divide radial and ulnar interosseous tendons proximal to the MCPJ. The sagittal hood fibres of the extrinsic extensor are identified and preserved while the transverse and oblique fibres of the intrinsic mechanism are released proximal to the MCP joint. The transverse portion of the intrinsic flexes the MCPJ.
Interosseous Muscle Slide/Fractional Lengthening
- Indication: residual intrinsic function from ischemic or spasticity.
- Technique: Elevate periosteal origins of dorsal and volar interossei from metacarpals ± first dorsal interosseous attachment to the thumb metacarpal. Splint MCP joints in full extension to allow the origin to heal distally.
- Tip: fractional lengthening is an alternative option. Obliquely incise the tendinous part of the myotendinous junction, preserving the muscular portion.
Ulnar Neurectomy
- Indication: spastic patients without volitional control.
- Technique: Excise the ulnar nerve's motor branch in the Guyon canal. Index/middle lumbricals remain slightly active.
- Note: In pronounced spasticity, extrinsics can overshadow intrinsic tightness. Post-extrinsic release, if MCP extends passively, neurectomy halts intrinsic contracture. If not, tenotomy near MCP aids extension.
Swan-Neck Deformity
Chronic intrinsic tightness results a swan neck deformity with volar plate laxity.
Intrinsic Tenodesis
- Indication: swan neck deformity due to chronic PIPJ hyperextension.
- Technique: Distal release of tighter intrinsic, reroute contralateral intrinsic tendon beneath the Cleland ligament to counteract hyperextension. Secure the tendon to the proximal phalanx after tenotomizing at its proximal third.
- Tip: a lateral band translocation can be performed if concerns regarding Cleland ligament's strength in holding volarly-positioned lateral bands. Divide Cleland, locate the volar plate and flexor sheath, create a dorsal flap, translocate the lateral band volar, and reposition the flap anatomically.
Lateral Band Mobilisation
- Indication: Rigid swan neck deformity.
- Technique: extensor tenolysis, dorsal capsulectomy, and lateral band mobilization via a dorsal incision. Release lateral bands from central slip and triangular ligament.
Lumbrical-plus Finger
Radial Lateral Band Resection
- Indication: lumbrical plus finger resulting from lumbrical tightness.
- Technique: Transect radial lateral band at the origin (palm) or insertion (dorsal apparatus) to mitigate paradoxical extension.
Conclusion
1. Intrinsic Plus Hand Definition: Gained a comprehensive understanding of the Intrinsic Plus condition, its historical background by Finochietto and Bunnell, and its clinical presentation of tight interossei and lumbricals causing characteristic hand deformities.
2. Intrinsic Muscle Anatomy and Function: Learned about the anatomy of interossei and lumbricals, their contribution to hand movement, grip, and pinch strength, and how their dysfunction leads to the Intrinsic Plus hand.
3. Intrinsic Plus Aetiology: Recognized the various local and systemic causes of intrinsic tightness, including fractures, Rheumatoid Arthritis, and other conditions affecting the interosseous muscles.
4. Diagnostic Approach to Intrinsic Plus Hand: Gained knowledge on diagnosing the Intrinsic Plus hand, particularly through Bunnell's Test, and understanding the potential progression to non-correctible contractures and swan-neck deformities.
5. Non-Surgical and Surgical Management: Explored non-surgical treatment options aimed at preventing irreversible contractures and looked into the surgical management of the Intrinsic Plus hand, understanding the procedures available depending on the severity and specific joint affected.
Further Reading
- Akhavani MA, Paleolog EM, Kang N. Muscle hypoxia in rheumatoid hands: does it play a role in ulnar drift? J Hand Surg Am. 2011 Apr;36(4):677-85. doi: 10.1016/j.jhsa.2011.01.035. PMID: 21463729.
- Brand PW. Clinical mechanics of the hand. 1985
- BUNNELL S, DOHERTY EW, CURTIS RM. Ischemic contracture, local, in the hand. Plast Reconstr Surg (1946). 1948 Jul;3(4):424-33. doi: 10.1097/00006534-194807000-00004. PMID: 18874816.
- Zancolli E. Structural and dynamic bases of hand surgery. 1979.
- Espiritu MT, Kuxhaus L, Kaufmann RA, Li ZM, Goitz RJ. Quantifying the effect of the distal intrinsic release procedure on proximal interphalangeal joint flexion: a cadaveric study. J Hand Surg Am. 2005 Sep;30(5):1032-8. doi: 10.1016/j.jhsa.2005.05.003. PMID: 16182064.
- Finochietto R. Retraccion de volkmann de los musculos intrinsecos de la mano. 1920.
- Kozin SH, Porter S, Clark P, Thoder JJ. The contribution of the intrinsic muscles to grip and pinch strength. J Hand Surg Am. 1999 Jan;24(1):64-72. doi: 10.1053/jhsu.1999.jhsu24a0064. PMID: 10048518.
- Lauer RT, Kilgore KL, Peckham PH, Bhadra N, Keith MW. The function of the finger intrinsic muscles in response to electrical stimulation. IEEE Trans Rehabil Eng. 1999 Mar;7(1):19-26. doi: 10.1109/86.750547. PMID: 10188604.
- Paksima N, Besh BR. Intrinsic contractures of the hand. Hand Clin. 2012 Feb;28(1):81-6. doi: 10.1016/j.hcl.2011.10.001. PMID: 22117926.
- Parkes A. The "lumbrical plus" finger. J Bone Joint Surg Br. 1971 May;53(2):236-9. PMID: 5578219.
- Schweitzer TP, Rayan GM. The terminal tendon of the digital extensor mechanism: Part I, anatomic study. J Hand Surg Am. 2004 Sep;29(5):898-902. doi: 10.1016/j.jhsa.2004.04.022. PMID: 15465241.
- Seu M, Pasqualetto M. Hand therapy for dysfunction of the intrinsic muscles. Hand Clin. 2012 Feb;28(1):87-100. doi: 10.1016/j.hcl.2011.09.001. PMID: 22117927.
- Stack, H. G. (1962). MUSCLE FUNCTION IN THE FINGERS. The Journal of Bone & Joint Surgery British Volume, 44-B(4), 899-909. https://doi.org/10.1302/0301-620X.44B4.899
- Tafti MA, Cramer SC, Gupta R. Orthopaedic management of the upper extremity of stroke patients. J Am Acad Orthop Surg. 2008 Aug;16(8):462-70. doi: 10.5435/00124635-200808000-00005. PMID: 18664635.
