

Summary Card
Definition of Polydactyly
Congenital duplication of digits that can be radial, ulnar, or central.
Overview of Radial Polydactyly
A pre-axial duplication of the thumb classified by Wassell.
Overview of Ulnar Polydactyly
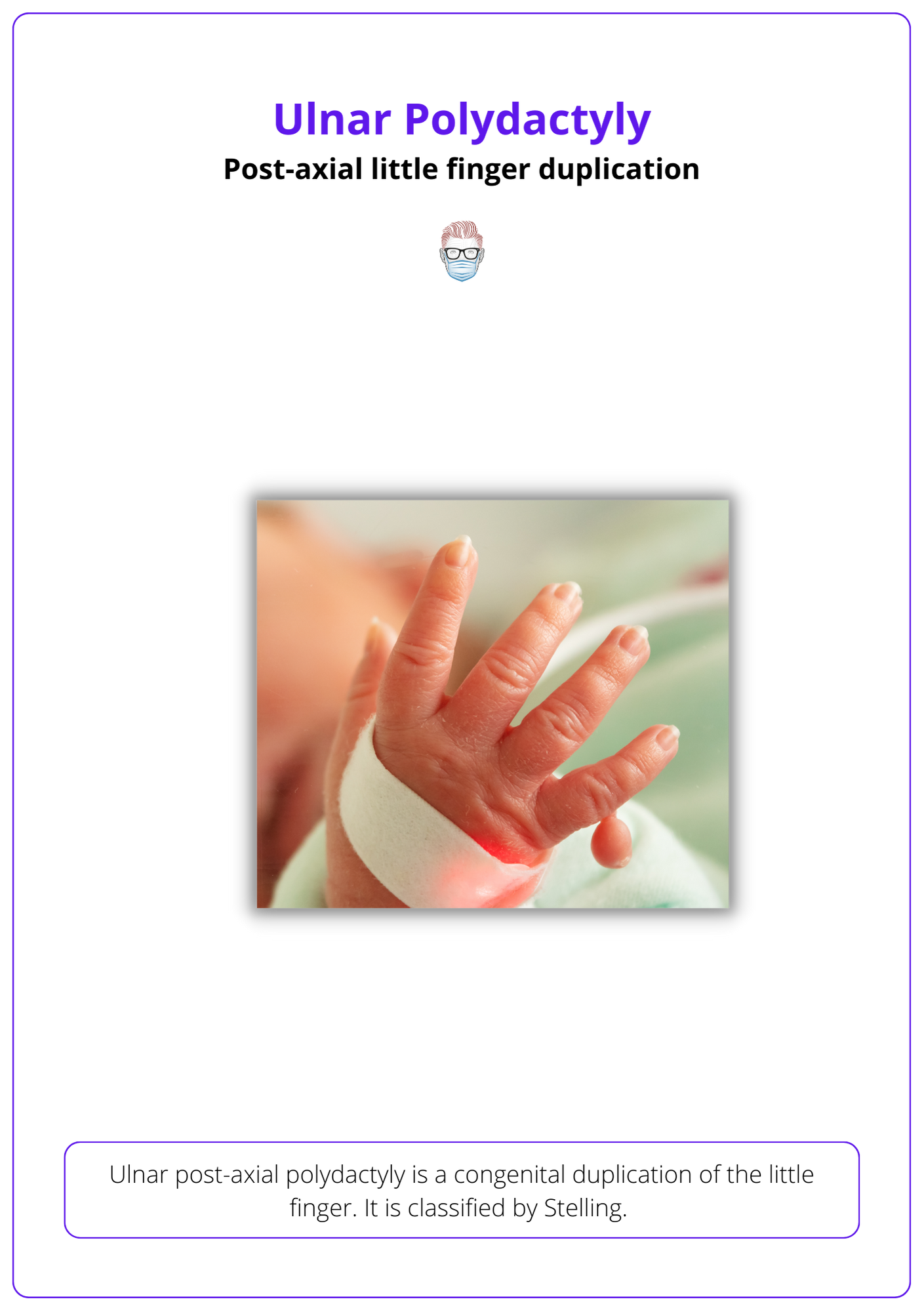
Post-axial duplication of little finger classified by Stelling.
Definition of Polydactyly
Polydactyly is a congenital duplication of a finger. It can be pre-axial (radial), central and post-axial (ulnar) and is caused by disruption at the ZPE and AER embryological signalling zones.
The image below shows the congenital duplication of a finger.
Overview of Radial Polydactyly
A pre-axial duplication of the thumb classified by Wassell.
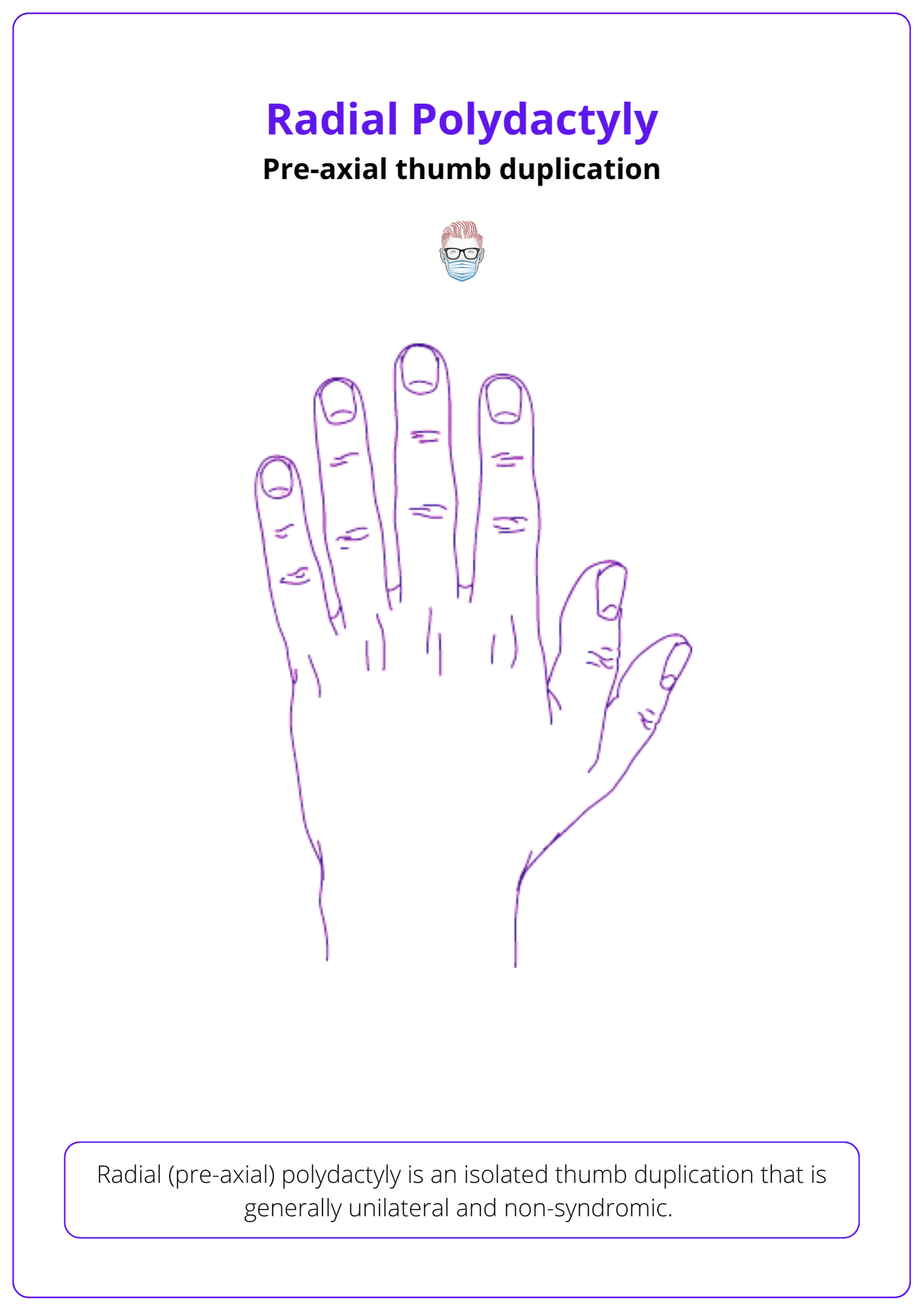
Radial (pre-axial) polydactyly is an isolated thumb duplication that is generally unilateral and non-syndromic. From a demographic perspective, it is different from ulnar polydactyly because:
- It is usually sporadic.
- It primarily affects Caucasians.
- Patients should be screened for Fanconi anaemia.
The image below shows an overview of radial polydactyly.
Classification of Radial Polydactyly
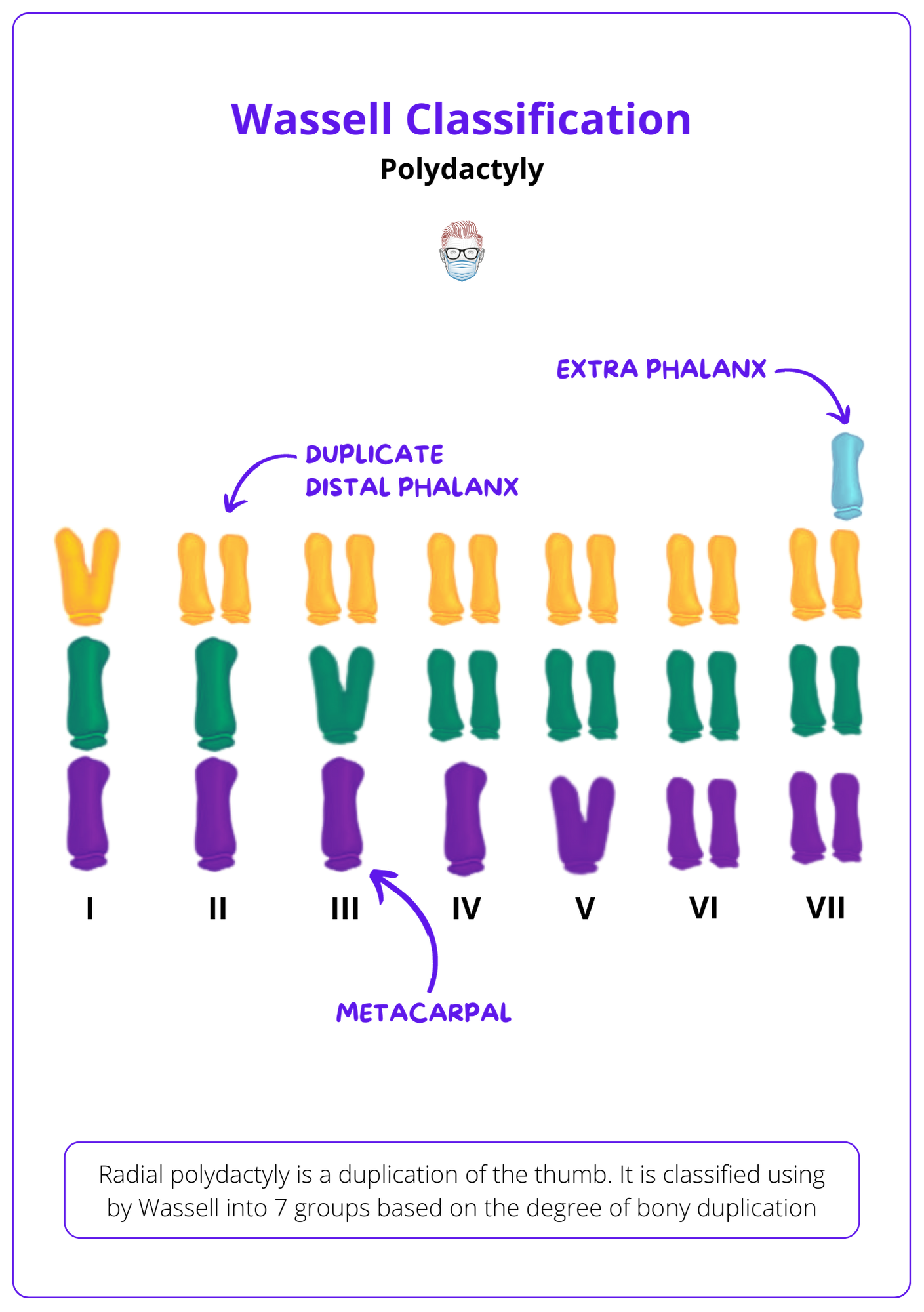
Radial polydactyly is a duplication of the thumb. It is classified by Wassell into 7 groups based on the degree of bony duplication. Type IV is the most common radial polydactyly.
- Type I: Bifid Distal Phalanx
- Type II: Duplicate Distal Phalanx
- Type III: Bifid Proximal Phalanx + Duplicate Distal Phalanx
- Type IV: Duplicate Distal Phalanx + Duplicate Distal Phalanx
- Type V: Bifid 1st metacarpal + Duplicate Distal and Proximal Phalanx
- Type VI: Duplicate 1st metacarpal + Distal Phalanx + Proximal Phalanx
- Type VII: Triphalangeal thumb (triangular or rectangular extra middle phalanx) + normal thumb
Diagnose triphalangeal thumb by excluding a five-finger hand. Look at the nail position (not in normal pronation) and x-ray (extra finger metacarpal). Surgery includes pollicisation and web space creation.
This Wassell classification of radial polydactyly is illustrated below.
Management of Radial Polydactyly
Key Principles
Surgery aims to create an anatomically aligned thumb with joint stability that enables function. Ideally, it is performed prior to developing the thumb-pinch index at age 1.
A decision should be made on which duplicate to retain. This can be guided by:
- Size: one duplicate is usually hypoplastic or rudimentary.
- Function: ulnar collateral ligament is important for pinch.
- Movement: passive and active range of movement.
- Radiology: location of duplication.
The Wassell classification notes "equal parts" or "spare parts" surgery.
"Equal parts surgery"
The Bilhaut-Cloquet Technique is indicated in Types I + II or convergent and symmetrical type IV polydactyly. Excise adjacent inner halves of each duplicate and fuse the remaining outer segments.
- Standard Technique: simple wedge excision of structures.
- Modified Technique: preservation of one nail complex and physics of one of the duplicates.
Nail problems, epiphysiodesis and reduced range of movement limit this technique.
Pre-axial polydactyly is illustrated in the image below.
"Spare Parts Surgery"
This is indicated in types III and IV or asymmetrical I and II. Excise one duplicate and reconstruct the other using "spare parts surgery" in a single operation. This should be done before the patient turns 1 year of age before they develop the thumb-index pinch.
The key steps to my operation are:
- Incision: avoid straight lines to prevent full extension/flexion, and the nail bed to reduce the risk of nail plate ridging.
- Excision: excise radial duplicate (proximal and smaller than ulnar digit).
- Ligaments: reconstruct radial collateral ligament of IPJ with a periosteal slave from the excised digit (Manske), preserve RCL of thumb MCPJ.
- Tendons: realign EPL insertion to form a single tendon, centralise FPL by reconstructing the pulley, and transfer APB insertion from the radial duplicate.
- Bone: excise asymmetric joint surfaces, closed wedge osteotomy of proximal phalanx, trans-articular 0.6 or 0.7mm K-wire for 4 weeks.
These patients can be discharged same day if the patient is well and followed up in a specialist hand therapy clinic.
Additional Techniques
- Types V + VI also requires web space reconstruction, intrinsic reconstruction, basal joints and metacarpal osteotomies.
- Type VII requires treatment of the extra interphalangeal joint. If a delta phalanx is present, it is excised, and soft tissue is reconstructed. If the extra phalanx is rectangular, chrondresis of the least mobile joint.
The surgical correction of radial polydactyly is shown in the video below.
Overview of Ulnar Polydactyly
Post-axial duplication of little finger classified by Stelling.
Ulnar post-axial polydactyly is a congenital duplication of the little finger digits. Unlike radial polydactyly, it is commoner in African American males and is more often bilateral. It is usually autosomal dominant with variable penetrance.
The image below shows an overview of Ulnar Polydactyly.
Classification of Ulnar Polydactyly
Ulnar polydactyly can be described using Stelling's classification. It also guides management.
- I: "Nubbin" - soft tissue without bone excised or ligated as a neonate.
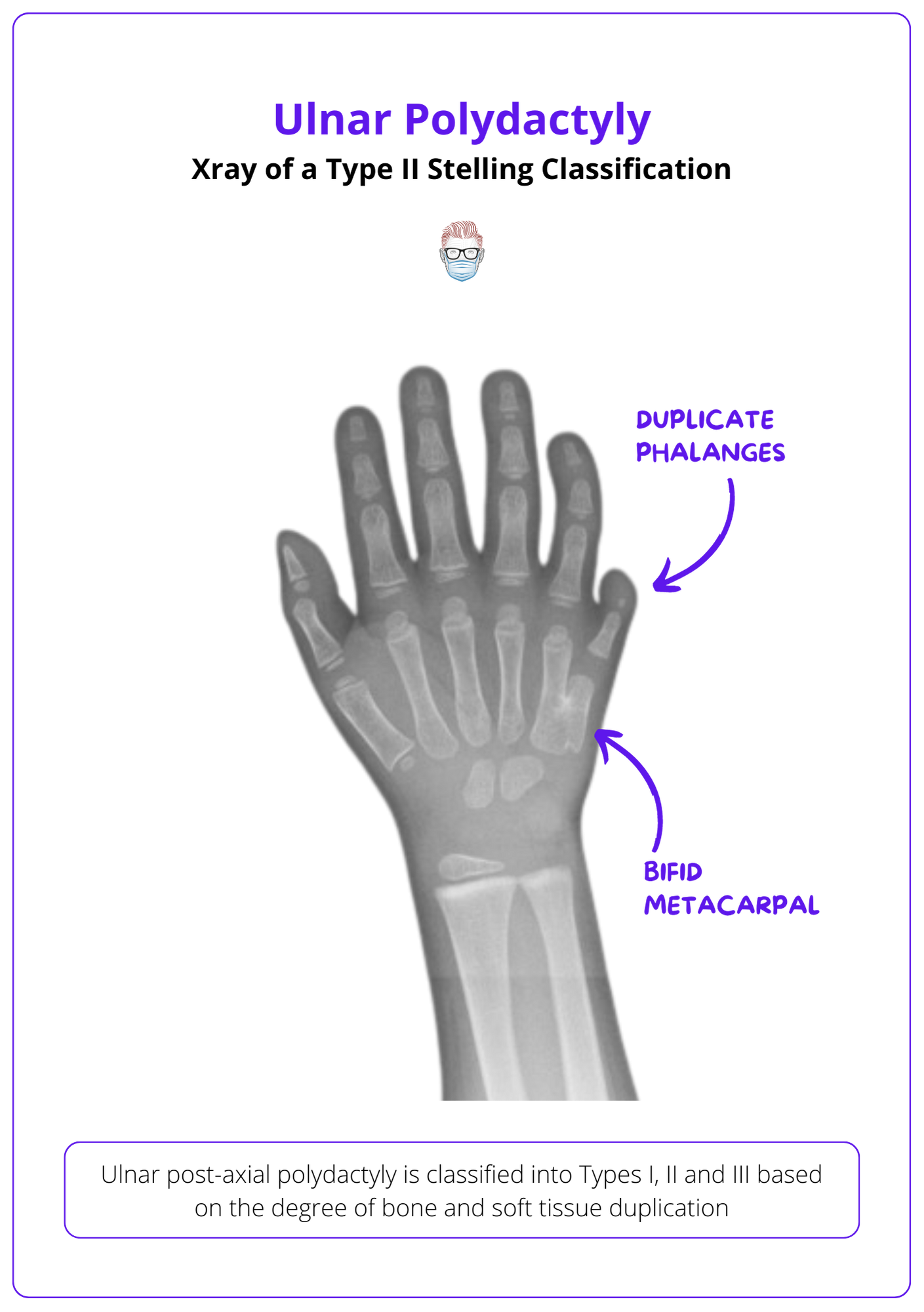
- II: extra digit is structurally complete and articulates with normal or bifid metacarpal or phalanx.
- III: extra digit is structurally complete and has its metacarpal.
Types II and III patients require resection and reconstruction. This involves the abductor digit minimi and ulnar collateral ligament attachments to be transferred to the adjacent finger.
An alternative classification can be Type A (well-developed supernumerary digit) or Type B (digit is rudimentary and pedunculated).
The image below illustrates an X-ray representation of type II Selling Classification.
Conclusion
1. Basic Understanding of Polydactyly: You have learned that polydactyly involves the congenital duplication of digits and can occur as radial, central, or ulnar types, each with unique characteristics and genetic implications.
2. Polydactyly Classification Systems: You now understand the classifications for radial and ulnar polydactyly, which include the Wassel classification for radial polydactyly and the Stelling classification for ulnar polydactyly.
3. Surgical Management Approaches: The article has provided insights into the surgical techniques for correcting radial and ulnar polydactyly, highlighting the importance of choosing the appropriate procedure based on the type and severity of the duplication.
4. Genetic and Embryological Aspects: You have become familiar with the genetic mutations and embryological disruptions that lead to polydactyly, deepening your understanding of its developmental origins and the associated syndromes.
