

Summary Card
Definition
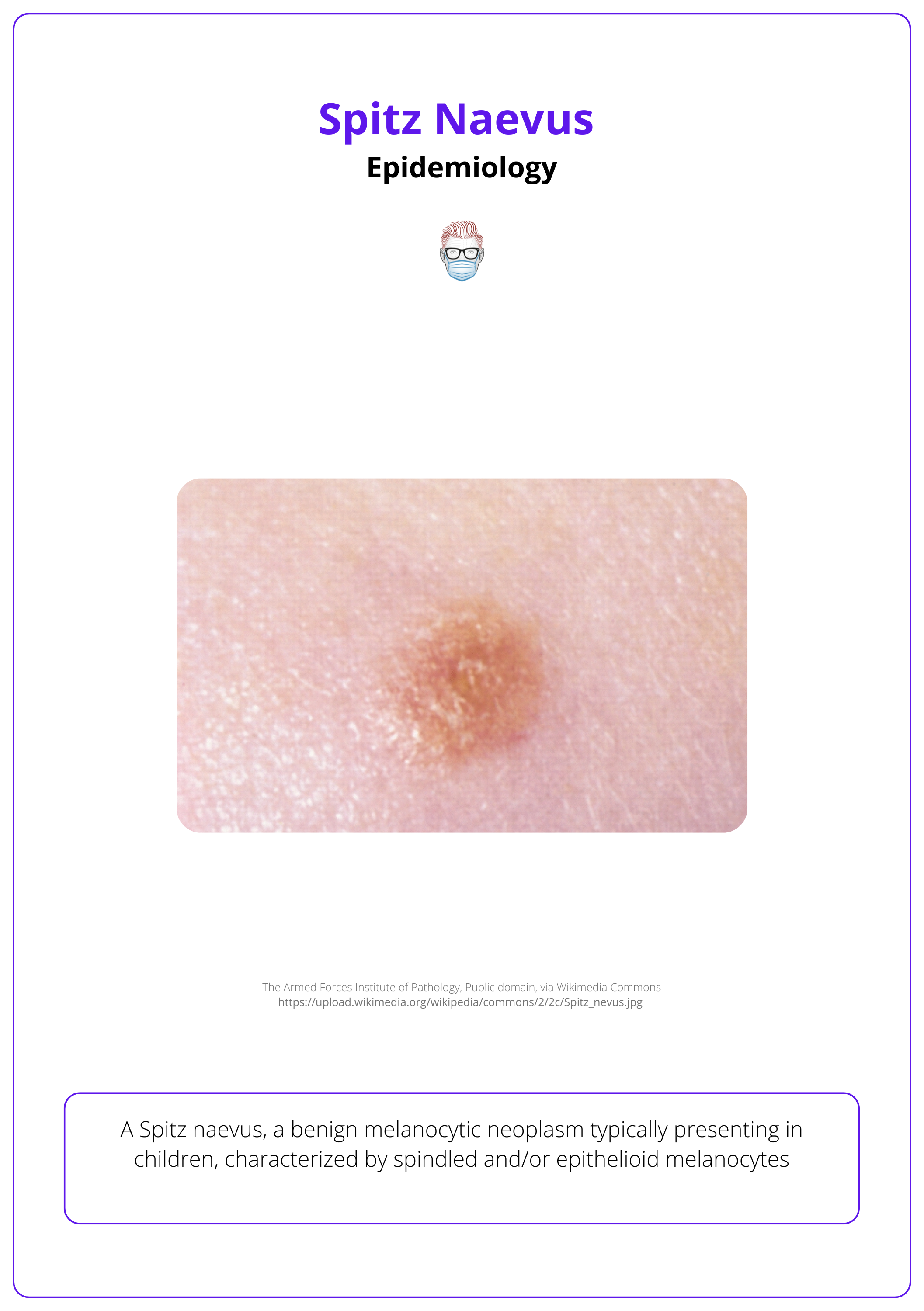
Spitz nevus is a rare, benign melanocytic nevus, representing about 1% of surgically removed childhood nevi. It mostly affects children.
Pathophysiology
Spitz naevi have unique histological traits, including larger melanocytes and Kamino bodies. Variants include classic, spindle cell, pigmented, and atypical forms
Clinical Features
Spitz nevi appear as single, dome-shaped papules with uniform pigmentation. They exhibit starburst or globular patterns on dermoscopy and undergo rapid growth, followed by long-term stability and potential spontaneous regression.
Atypical Spitz Tumour and Spitzoid Melanoma
Atypical Spitz tumors have features between benign and malignant. Spitzoid melanoma resembles benign nevi but behaves like melanoma, with a generally better prognosis.
Management
Management involves non-surgical monitoring for children under 12 and excision biopsy for older children, adults, or changing lesions.
Primary Contributor: Dr Kurt Lee Chircop, Educational Fellow.
Reviewer: Dr Waruguru Wanjau, Educational Fellow.
Definition of Spitz Naevus
Spitz naevus is a benign melanocytic neoplasm that commonly presents in the paediatric population.
Spitz naevus is a distinct clinical and histological type of melanocytic nevus, characterised by a benign tumour formation of spindled and/or epithelioid melanocytes.
A spitz naevus represents about 1% of naevi surgically removed in childhood.
Originally described as ‘melanomas of childhood’ by Spitz in 1948, it was later found that 12 of the original 13 cases were benign. Only one case was a true melanoma that spread and caused death (Spitz, 2019).
Over the years multiple names have been used including Spitz naevus, Spitz tumour, spindle cell naevus, and epithelioid naevus.
Pathophysiology of Spitz Naevus
Many variants of Spitz naevus exist, sharing common histological findings including spindled and epithelioid melanocytes and Kamino bodies.
In Spitz naevi, like other types of naevi and melanoma, cell growth is mainly driven by mutations in genes within the RAS-RAF-MEK-ERK-MAP kinase pathway.
Spitz naevus is a type of melanocytic naevus that meets all the key histological criteria for diagnosing a melanocytic naevus but has unique features that set it apart. Histologically, Spitz naevi consist of:
- Spindled and/or epithelioid melanocytes
- Larger melanocytes than those found in other types of naevi.
- Kamino bodies (PAS-positive eosinophilic globules), which are unique to Spitz naevi (Gaspar, 2020).
Clinical Features of Spitz Naevus
Spitz naevus typically presents as a single, well-defined, non-ulcerated papule with varying pigmentation, showing characteristic patterns on dermoscopy.
General Appearance
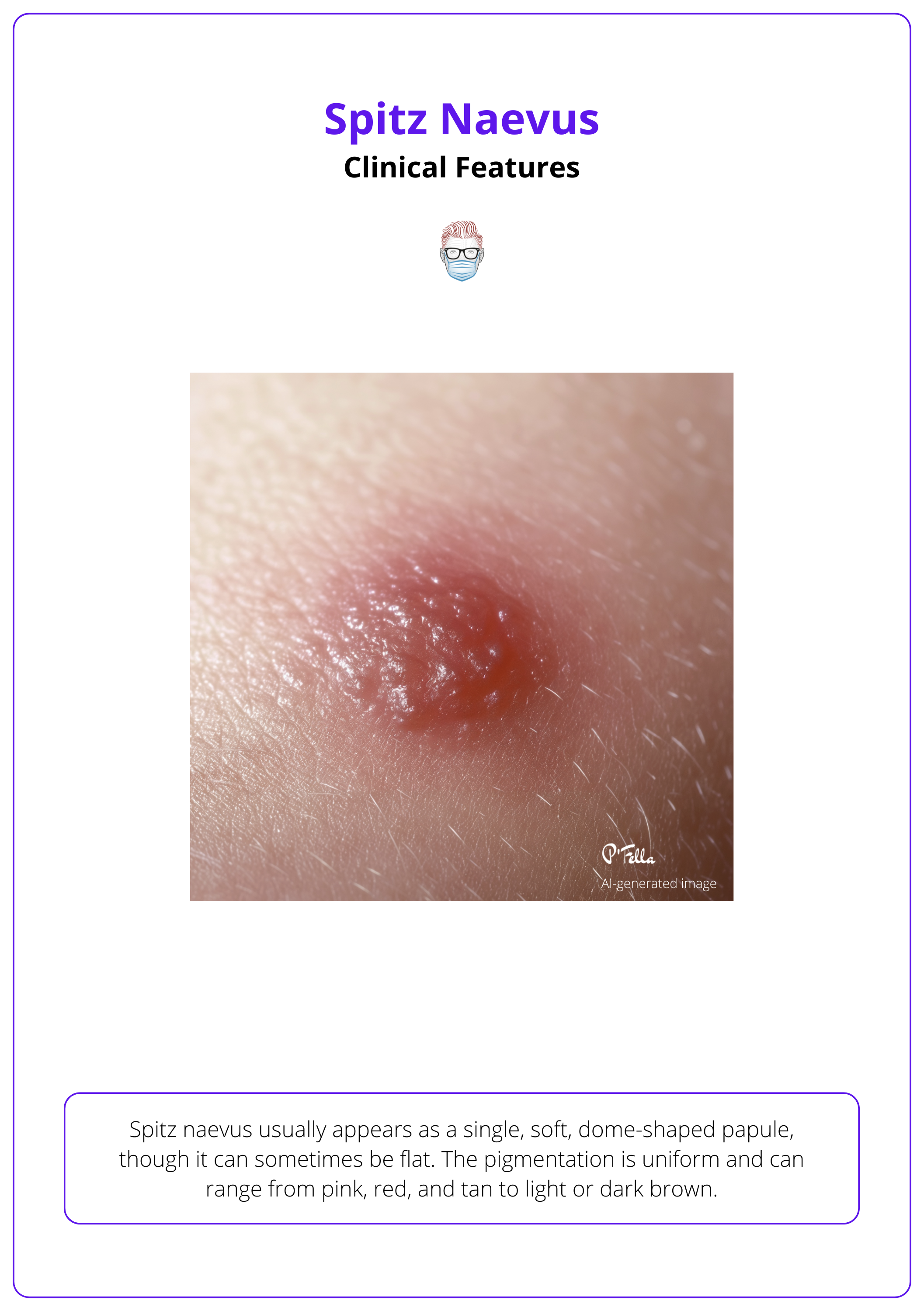
Spitz naevus usually appears as a single, soft, dome-shaped papule, though it can sometimes be flat. The pigmentation is uniform and can range from pink, red, and tan to light or dark brown. Variants with ALK fusions may exhibit colors from amelanotic to darkly pigmented.
Common clinical features of the subtypes include:
- Size: Typically ranges from 0-2 cm in diameter.
- Location: Commonly found on the face or limbs.
- Presentation: Generally presents as solitary lesions, though multiple lesions can occur.
- Growth Pattern: Rapid growth phase lasting a few months, followed by a static phase that may last for years.
- Regression: Lesions may regress and disappear spontaneously over time. (Argenziano, 2011).
In patients with severe solar elastosis and elderly individuals, diagnosis of Spitz naevus should be made cautiously, as such lesions in this cohort of patients are more likely to be malignant in nature.
Types of Spitz Naevi
- Classic Spitz Naevus: Symmetric, dome-shaped lesions with uniform pink or tan coloration and distinct borders. These are composed of spindle or epithelioid melanocytes.
- Spindle Cell Tumour of Reed: Features elongated spindle-shaped melanocytes arranged in a nodular, fascicular pattern.
- Pigmented Spitz Naevus: Displays varying pigmentation from light brown to black, potentially mimicking melanoma both clinically and histologically.
- Atypical Spitz Naevus/Tumour: Shows atypical features that differ from typical Spitz naevi, often requiring careful evaluation.
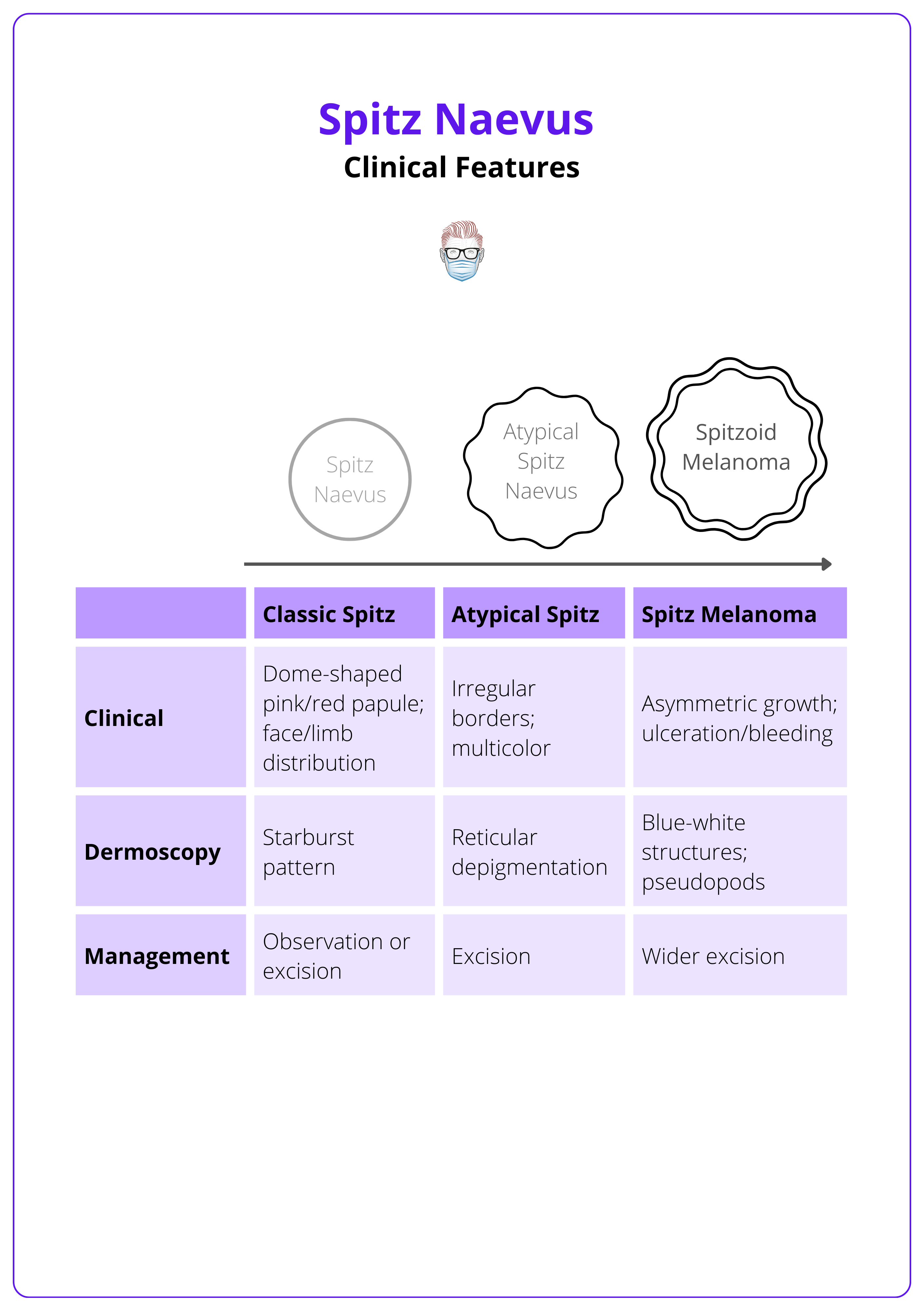
These types, their characteristics, and management options are summarized in the table below.
Agminated Spitz naevus is a rare entity that presents with multiple Spitz naevi in a segmental presentation. It is an example of cutaneous mosaicism and is due to a genetic mutation.
Dermoscopy Findings
- Starburst Pattern: Radial streaks or lines extending from the periphery, highly indicative of Spitz nevi.
- Globular Pattern: Round, oval, or cobblestone-like structures, uniformly distributed and colored.
- Symmetric Pigmentation: Evenly distributed pigmentation within the lesion, giving it a benign appearance.
- Central Homogeneous Area: A uniformly colored and textured area in the center of the lesion
The dermoscopic findings of spitz naevi are summarised in this video below.
Atypical Spitz Tumour and Spitzoid Melanoma
Atypical Spitz tumour is an intermediate entity that has features common to both benign Spitz naevi and melanoma. Spitzoid melanoma is a conventional melanoma that resembles Spitz tumours in histology.
Atypical Spitz Tumour
Atypical Spitz Tumour (AST) is a special type of Spitz naevus. While it has a higher risk of involving sentinel nodes, it usually behaves less aggressively (Harms, 2015).
These tumors consist of epithelioid and spindled melanocytes. They have enough atypical features to stand out from standard Spitz nevi but not enough to be classified as melanoma. ASTs are seen as an intermediate stage between typical Spitz naevus and Spitzoid melanoma
- Appearance: ASTs are usually raised, dome-shaped, and have a smooth surface. They are often larger than common moles.
- Location: Commonly found on the lower limbs, but they can appear anywhere on the body.
- Shape: Typically symmetrical with well-defined borders, although they can sometimes have irregular edges.
- Color: The color can vary widely, including pink, red, tan, brown, or black, and may have mixed pigmentation within the same lesion.
- Age: Mostly seen in children and adolescents, but they can occur at any age (Harms, 2015)
- Treatment: ASTs should be conservatively excised if atypical features are noted (Harms, 2015)
Spitzoid Melanoma
Spitzoid melanoma is a rare type of malignant melanoma that closely resembles the benign neoplasm Spitz naevus in its histology (Batra, 2015).
Clinical Features of Spitzoid Melanoma:
- Appearance: typically presents as a changing and enlarging papule or nodule. It may appear amelanotic or pigmented. Advanced stages of the condition might show crusting and ulceration.
- Location: most commonly found on the head or extremities.
- Shape and Colour: often appear round and uniform in colour without the classic ABCDE characterisitics.
- Origin: It can develop as a new lesion (de novo) or evolve from an existing Spitz naevus.
Spitzoid Melanoma should be managed as any other cutaneous melanoma and staged accordingly. However, it carries a much better prognosis (Paradela, 2013).
When suspicious lesions are biopsied, histological analysis may yield uncertain results, and a diagnosis of Spitzoid Melanoma of Uncertain Malignant Potential (STUMP) may be considered.
Management of Spitz Naevus
Management depends on the patient's age and characteristics of the lesion. It ranges from active observation to surgical excision to obtain a histological diagnosis.
Spitz naevi represent a benign neoplasm and aggressive surgical management is not usually warranted if the diagnosis is certain, especially in the paediatric population or when cosmetic areas of the face are involved.
Observation (Children <12 years)
- monitored through digital dermatoscopic surveillance.
- tracking changes in the lesion's dermatoscopic appearance with serial photographs.
- 3 monthly follow-up appointments until growth ceases.
- 6 monthly or yearly follow-ups until resolution.
- Excision biopsy if changes are observed on follow-up (Lallas, 2017).
Surgical Management
This method is used for children above 12 years and adults, in case of an evolving lesion.
- Incision biopsy in large lesions in cosmetically sensitive areas.
- Punch biopsy (not recommended in view of diagnostic inaccuracy).
- Excision biopsy with 2-3 mm margin for histological evaluation (preferred).
- Wide excision with a further margin of confirmed atypical Spitz tumours (regardless of complete excision at biopsy) (Ludgate, 2009).
Conclusion
1. Understanding of Spitz Nevus: You've gained insights into the nature and characteristics of Spitz nevus, including its definition, epidemiology, and the typical demographic affected.
2. Histopathological Features: You've learned about the unique histological traits of Spitz nevi, such as larger melanocytes and the presence of Kamino bodies, and how these features differentiate various subtypes.
3. Clinical Presentation: You are now familiar with the clinical appearance of Spitz nevi, how they present as dome-shaped papules with uniform pigmentation, and their behavior through growth phases.
4. Atypical Spitz Tumors and Spitzoid Melanoma: You've explored atypical Spitz tumors and Spitzoid melanoma, understanding their intermediate and malignant behaviors respectively, and how they compare to benign Spitz nevi.
5. Comprehensive Management: You understand the varied management strategies for Spitz nevi, ranging from non-surgical monitoring in younger patients to surgical excision in older children and adults based on lesion changes.
Further Reading
- Sainz-Gaspar L, Sánchez-Bernal J, Noguera-Morel L, Hernández-Martín A, Colmenero I, Torrelo A. Spitz Nevus and Other Spitzoid Tumors in Children -Part 1: Clinical, Histopathologic, and Immunohistochemical Features. Actas Dermosifiliogr (Engl Ed). 2020 Jan 2;111(1):7-19. English, Spanish. doi: 10.1016/j.ad.2019.02.011. Epub 2019 Nov 28. PMID: 31787210.
- What to look for: ABCDEs of melanoma. American Academy of Dermatology www.aad.org Accessed on 11th May 2024
- Spitz K, Piliang M, Mostow E. Sophie Spitz: A woman ahead of her time. Int J Womens Dermatol. 2019 Mar 11;5(3):190-191. doi: 10.1016/j.ijwd.2019.02.002. PMID: 31360758; PMCID: PMC6637087.
- Argenziano G, Agozzino M, Bonifazi E, Broganelli P, Brunetti B, Ferrara G, Fulgione E, Garrone A, Zalaudek I. Natural evolution of Spitz nevi. Dermatology. 2011;222(3):256-60. doi: 10.1159/000326109. Epub 2011 Apr 13. PMID: 21494025.
- A. Lallas, Z. Apalla, D. Ioannides, E. Lazaridou, A. Kyrgidis, P. Broganelli, R. Alfano, I. Zalaudek, G. Argenziano, on behalf of the International Dermoscopy Society, Renato Bakos, Andreas Blum, Ralph Braun, Horacio Cabo, Allan Halpern, Rainer Hofmann‐Wellenhof, Harald Kittler, Josep Malvehy, Ashfaq Marghoob, Scott Menzies, Elvira Moscarella, John Paoli, Giovanni Pellacani, Susana Puig, Harold Rabinovitz, Alon Scope, Peter Soyer, Wilhelm Stolz, Masaru Tanaka, Luc Thomas, Philipp Tschandl, Update on dermoscopy of Spitz/Reed naevi and management guidelines by the International Dermoscopy Society, British Journal of Dermatology, Volume 177, Issue 3, 1 September 2017, Pages 645–655, https://doi.org/10.1111/bjd.15339
- Harms, K. L., Lowe, L., Fullen, D. R., & Harms, P. W. (2015). Atypical Spitz Tumors: A Diagnostic Challenge. Archives of pathology & laboratory medicine, 139(10), 1263–1270. https://doi.org/10.5858/arpa.2015-0207-RA
- Batra S. (2015). Spitzoid melanoma of childhood: a case series and review. Melanoma management, 2(2), 121–125. https://doi.org/10.2217/mmt.15.6
- Paradela S, Fonseca E, Pita-Fernández S, Prieto VG. Spitzoid and non-spitzoid melanoma in children: a prognostic comparative study. J Eur Acad Dermatol Venereol. 2013 Oct;27(10):1214-21. doi: 10.1111/j.1468-3083.2012.04686.x. Epub 2012 Aug 29. PMID: 22928628.
- Ludgate, M. W., Fullen, D. R., Lee, J., Lowe, L., Bradford, C., Geiger, J., Schwartz, J., & Johnson, T. M. (2009). The atypical Spitz tumor of uncertain biologic potential: a series of 67 patients from a single institution. Cancer, 115(3), 631–641. https://doi.org/10.1002/cncr.24047
- Situm, M., Bolanca, Z., Buljan, M., Tomas, D., & Ivancić, M. (2008). Nevus Spitz--everlasting diagnostic difficulties--the review. Collegium antropologicum, 32 Suppl 2, 171–176.
- Metzger AT, Kane AA, Bayliss SJ. Differences in treatment of Spitz nevi and atypical Spitz tumors in pediatric patients among dermatologists and plastic surgeons. JAMA Dermatol. 2013 Nov;149(11):1348-50. doi: 10.1001/jamadermatol.2013.4947. PMID: 24026360.
