
In this week's edition
- ✍️ Letter from P'Fella
4 Tips for the FRCS Viva - 🤓 The Sunday Quiz
How well do you know congenital dermoid cysts? - 🎙️ Behind the 'Fella
Underrated Plastic Surgery Resources Every Surgeon Needs - 🖼️ Anatomy Illustration of the Week
Anatomy of hard and soft palate. - 🎓 theFellow's Corner
This week's feature: Macrodactyly. - 📖 What Does the Evidence Say?
Should we operate on paediatric trigger thumbs? - 🔥 Articles of the Week
Pediatric trigger thumb, syndactyly surgical outcomes, & velopharyngeal dysfunction: 3 articles with 1 sentence summaries. - 💕 Feedback
Suggest ideas & give feedback!
A Letter from P'Fella
4 Tips for the FRCS Viva
With FRCS oral exams around the corner, I had a chat with Professor Andy Hart—an experienced examiner and JPRAS editor—who knows what it takes to pass the viva. Here are some tips you can put into action right now.
- Tip 1: Cut to the Chase
Skip the small talk—get straight to the diagnosis and management. “Examiners want to see you think like a consultant,” Andy says. Whether it’s melanoma or a surgical plan, go straight to the key points and show you’re in control. - Tip 2: Keep it Short and Sharp
Know when to stop. Give a precise answer and let it land. “Finish with a full stop,” Andy emphasizes. Don’t ramble—concise answers are what examiners are after. - Tip 3: Handle the Silence
Examiners might give no feedback, but don’t let that rattle you. Stay composed. “Keep the flow going,” Andy advises. Ask for details if needed, but stay focused and in charge of the case. - Tip 4: Practice Out Loud
You can’t just think your answers—say them out loud. Andy insists: “Practice mock exams, whether it’s with peers or by yourself.” Verbal practice builds confidence and clarity under pressure.
Our new Oral Exams feature has over 35+ real FRCS scenarios, with two added every week. Perfect for getting those last-minute reps in. Get ready to ace the exam.
Also, keep an eye out for my full conversation with Andy on Behind the 'Fella—packed with insights to help you go into the viva with confidence.
Lot of Love,
P'Fella ❤️
The Sunday Quiz
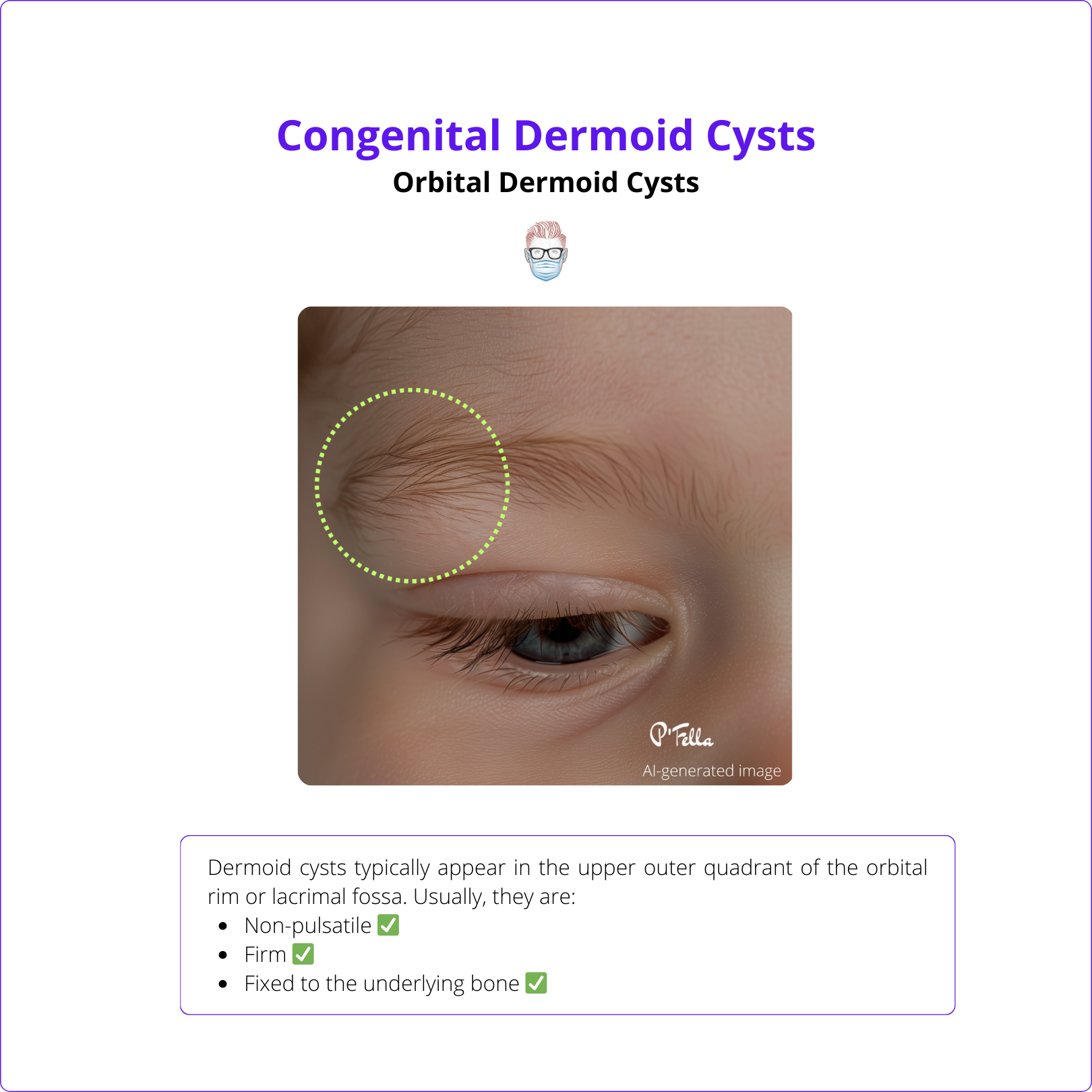
How Well Do You Know Congenital Dermoid Cysts?
Welcome to the next round of The Weekly Quiz.
Each edition of thePlasticsPaper includes a quiz question designed to challenge and engage our readers. Keep your wits about you and join in every week — the winner at the end of six rounds will earn you a $100 voucher.
Behind the ‘Fella
Underrated Plastic Surgery Resources Every Surgeon Needs
Tune into our podcast for exclusive team meetings where we uncover behind-the-scenes details of the platform and discuss hot topics in plastic surgery with our fellows.
In our upcoming episode, we discuss our favourite resources for plastic surgery learning.
You can listen now on Spotify & Apple!
Anatomy Illustration of the Week
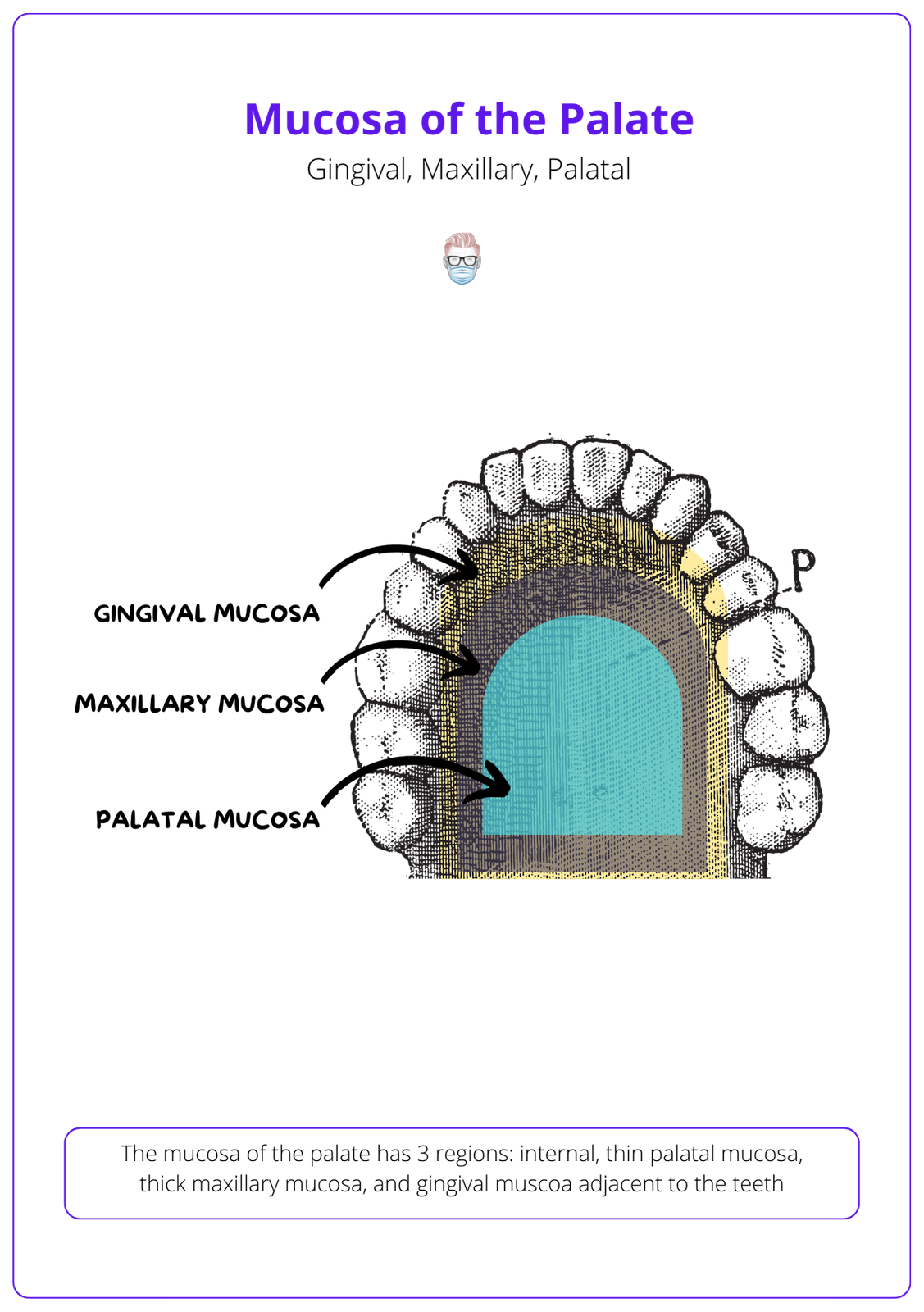
Anatomy of Hard and Soft Palate
In this new section, we feature an anatomical illustration. This edition looks at the anatomy of hard and soft palates.
👇
the Fellows' Corner
This Week's Focus: Macrodactyly
In case you've missed out, here's a reminder to check out our fresh articles, clinical cases, and surgical techniques.
Read below for an overview of our article on Macrodactyly.
Macrodactyly
Definition
Macrodactyly is the term for the overgrowth of a digit, out of proportion to the rest of the hand or foot.
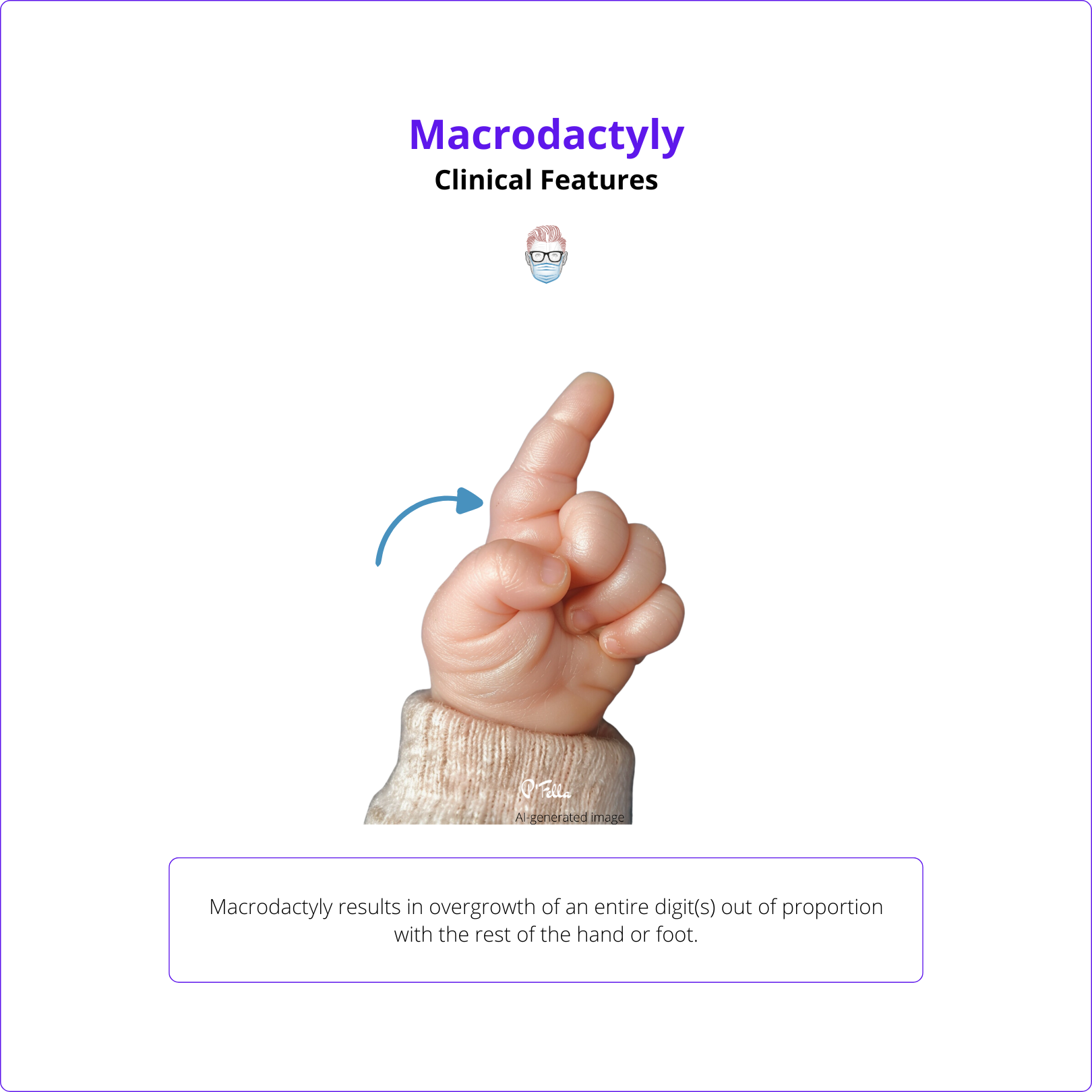
Clinical Features
Macrodactyly results in overgrowth of the entire digit(s) out of proportion with the rest of the hand or foot.
Investigations
X-rays, MRI, and gene analysis may be offered as part of the diagnostic process.
Management
Surgical management aims to stop overgrowth and debulk the digit. Addressing the nerve is important in reducing recurrence.
What Does the Evidence Say?
Should We Operate on Paediatric Trigger Thumbs?
Spontaneous recovery rates vary widely, from 12-66% (Dinham & Meggitt, 1974; Dunsmuir & Sherlock, 2000; Farr et al., 2014). Conservative treatments like splinting and passive exercises can be effective, with success rates of 55-67% (Farr et al., 2014). However, surgical release consistently demonstrates higher success rates of 95-100% (Farr et al., 2014; van den Borne et al., 2000; Marek et al., 2011). Complications from surgery are generally minor and rare (Marek et al., 2011; Dittmer et al., 2020).
Some studies suggest observing younger children for 6-12 months before considering surgery (Dinham & Meggitt, 1974; Dittmer et al., 2020). A network meta-analysis found splinting to be the most appropriate initial intervention, with open surgery recommended if conservative methods fail (Sirithiantong et al., 2020). Overall, treatment decisions should consider the child's age, thumb stage, and the potential for spontaneous recovery.
Articles of the Week
3 Interesting Articles with 1 Sentence Summaries
About one-third of pediatric trigger thumbs resolve naturally, but spontaneous resolution is less likely for severe interphalangeal joint flexion (>30°) and therefore benefits from early surgical intervention.
Simple syndactyly surgical outcomes revealed a low incidence of web creep, with most patients experiencing good scar quality, normal function, and minimal complications.
The effectiveness of ICG-A in enhancing tissue perfusion visualization, thus leading to better patient safety and reconstructive success in both mastectomy flaps and autologous procedures.
