

Summary Card
Definition
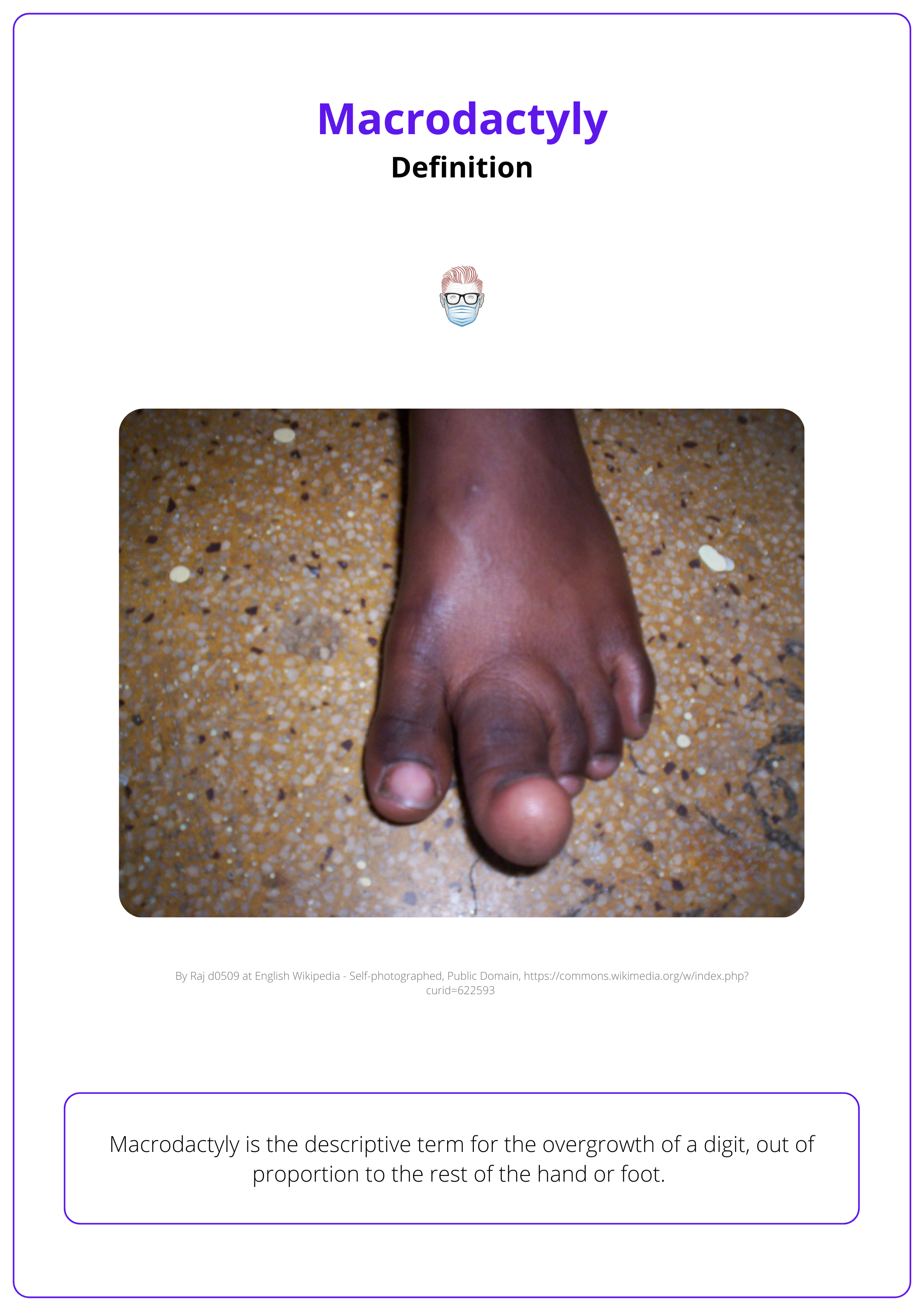
Macrodactyly is the term for the overgrowth of a digit, out of proportion to the rest of the hand or foot.
Clinical Features
Macrodactyly results in overgrowth of the entire digit(s) out of proportion with the rest of the hand or foot.
Investigations
X-rays, MRI, and gene analysis may be offered as part of the diagnostic process.
Management
Surgical management aims to stop overgrowth and debulk the digit. Addressing the nerve is important in reducing recurrence.
Primary Contributor: Dr Suzanne Thomson, Educational Fellow.
Reviewer: Dr Kurt Lee Chircop, Educational Fellow.
Definition of Macrodactyly
Macrodactyly is the descriptive term for the overgrowth of a digit, out of proportion to the rest of the hand or foot.
Macrodactyly is the disproportionate overgrowth of a digit, typically affecting one digit or nerve territory (e.g., thumb, index, and middle fingers in the median nerve territory). The majority are associated with lipofibromatosis of the nerve and a PiK3CA mutation (Wu, 2020).
It is classified into two types:
- Static: The enlarged digit maintains a consistent size difference relative to the rest of the hand or foot.
- Progressive: The enlarged digit grows more rapidly than the others.
It can occur in isolation or as part of a syndrome. It is a non-hereditary condition with no significant sex or geographical predilection. The image below illustrates macrodactyly of the foot.
Macrodactyly affects about 1 in 100,000 live births and accounts for approximately 1% of all upper limb congenital anomalies (Wu, 2020).
Clinical Features of Macrodactyly
Macrodactyly results in overgrowth of an entire digit(s) out of proportion with the rest of the hand or foot. It is usually noticed at birth.
Macrodactyly leads to the overgrowth of one or more digits, disproportionate to the rest of the hand or foot. It is usually unilateral and affects nerves and bones:
- Nerve: Typically affects one nerve territory, but can involve multiple in syndromic cases. Enlarged nerves may cause compression, like carpal tunnel
- Bone: Early osteophytes, osteoarthritis, & stiffness in the affected digit are common.
The image below illustrates macrodactyly of the index finger.

Bony overgrowth stops at physeal fusion, soft tissue grows into adulthood.
Classification
It is traditionally classified into four types, as described by Flatt and modified by Upton. Gigantism is combined with:
- Lipofibromatosis: common, associated with enlarged, fat-infiltrated nerves
- Neurofibromatosis: linked to plexiform neurofibromatosis, often bilateral
- Hyperostosis: rare, bony hyperostosis without nerve enlargement
- Hemihypertrophy: rare, hypertrophy of whole limb & intrinsic muscles, deformity with flexion contractures, ulnar deviation, adducted thumb
The index finger is most commonly affected by macrodactyly. Radial digits with macrodactyly deviate radially, while ulnar digits deviate ulnarly.
Associated Syndromes
Several syndromes also feature digital enlargement and are characterized by various associated symptoms.
- Neurofibromatosis: Café au lait spots, skin pigmentation, multiple neurofibromas, pedunculated skin lesions, ocular lesions.
- Ollier's Disease: Multiple enchondromas.
- Maffucci's Syndrome: Multiple enchondromas and hemangiomas.
- Parkes-Weber Syndrome: Limb hypertrophy, length discrepancies, capillary malformations, arteriovenous malformations.
- CLOVES Syndrome: Congenital lipomatous overgrowth, vascular malformations, epidermal nevi, scoliosis/spinal deformity.
- Klippel-Trenaunay-Weber Syndrome: Cutaneous hemangioma, atypical varicose veins, hemihypertrophy.
- Proteus Syndrome: Hamartomatous dysplasia, macrodactyly, pigmented linear epidermal nevi, subcutaneous hamartomas (Greens, 2011).
Macrodactyly occurs more often in the hands than the feet.
Investigations for Macrodactyly
X-rays, MRI, and gene analysis may be offered as part of the diagnostic process.
A standard workup for macrodactyly includes:
- Routine lab investigations
- X-ray to demonstrate growth plates and exostosis
- MRA/angiography for surgical planning
- Gene analysis, specifically for the Pi3KCA somatic mutation in severe cases
The image below illustrates the radiographical imaging of Macrodactyly of the hand.

Management of Macrodactyly
Surgical management aims to stop overgrowth and debulk the digit, with addressing the nerve being important to reduce recurrence.
The main goal in managing macrodactyly is to stop digit overgrowth before it surpasses adult size. Surgery is usually performed for functional and cosmetic reasons, while medical treatment is for refractory or extreme cases with Pi3KCA mutations.
Surgical Management
Surgical intervention requires thorough counseling due to the diffuse nature of the condition and its high likelihood of recurrence.
Limiting Growth Techniques:
- Ligation of Digital Arteries: Reduces blood supply to the digit.
- Compression Bandaging: Restricts growth.
- Epiphysiodesis: Arrests growth at the growth plate.
- Nerve Stripping and Nerve Resection: Reduces nerve-related growth and recurrence.
Debulking Procedures:
- Bone: Includes reducing osteotomies or removal of the middle phalanx.
- Soft Tissue: Involves excision of skin and fat, nail bed reduction. Techniques such as Tsuge’s method reduce length and bulk at the tip through a midlateral incision.
- Nerve Surgery: Stripping, resection, and decompression, especially for enlarged nerves traveling through the carpal tunnel.
- Liposuction: Useful for whole limb enlargement.
- Free Toe Transfer: Provides more functional and aesthetic digits, particularly in cases with syndactyly.
- Amputation: Ray amputation, with or without transposition, if the central digit is affected.
Medical Treatment
mTOR inhibitors like sirolimus are used to reduce tissue regeneration. This pathway is unchecked in cases with Pi3KCA mutations.
Following nerve resection, reconstruction may be performed to improve sensation and function (Kobreia, 2019).
Conclusion
1. Basics of Macrodactyly: Gained a comprehensive understanding of macrodactyly including its definition, pathophysiology related to genetic mutations, and the implications of nerve-associated overgrowth.
2. Clinical Presentation: Recognized the typical presentation patterns of macrodactyly and associated syndromic manifestations.
3. Diagnostic Approaches: Reviewed the necessary imaging and genetic tests used to confirm the diagnosis of macrodactyly, which assists in differentiating it from other digital anomalies.
4. Treatment Strategies: Explored surgical and medical treatment options aimed at managing overgrowth, addressing functional impairments, and minimizing aesthetic concerns.
5. Management of Complications: Discussed potential complications, particularly the recurrence of growth post-surgery, and strategies to mitigate these risks.
Further Reading
- Ms Gill Smith BFIRST/BSSH Global webinar - Congenital hand on YouTube
- Ezaki M, Beckwith T, Oishi SN. Macrodactyly: decision-making and surgery timing. J Hand Surg Eur Vol. 2019 Jan;44(1):32-42. doi: 10.1177/1753193418796441. Epub 2018 Sep 12. PMID: 30208752.
- Kobraei EM, Dusch MN, Meisel EM, Stevanovic M. A Novel Method of Treatment of Macrodactyly with Digital Nerve Resection and Nerve Allograft. Plast Reconstr Surg Glob Open. 2019 Oct 29;7(10):e2483. doi: 10.1097/GOX.0000000000002483. PMID: 31772904; PMCID: PMC6846287.
- Ezaki M. Insights into the pathogenesis of macrodactyly. J Hand Surg Eur Vol. 2019 Jan;44(1):25-31. doi: 10.1177/1753193418790928. Epub 2018 Aug 7. PMID: 30086673.
- Wu J, Tian G, Ji Y, Higgins JP, Lee WPA. Clinical Characteristics of 90 Macrodactyly Cases. J Hand Surg Am. 2020 Oct;45(10):982.e1-982.e5. doi: 10.1016/j.jhsa.2020.03.002. Epub 2020 Apr 13. PMID: 32299688.
- Bernhard SM, Adam L, Atef H, Häberli D, Bramer WM, Minder B, Döring Y, Laine JE, Muka T, Rössler J, Baumgartner I. A systematic review of the safety and efficacy of currently used treatment modalities in the treatment of patients with PIK3CA-related overgrowth spectrum. J Vasc Surg Venous Lymphat Disord. 2022 Mar;10(2):527-538.e2. doi: 10.1016/j.jvsv.2021.07.008. Epub 2021 Aug 3. PMID: 34358672.
- Green DP, Wolfe SW. Green’s Operative Hand Surgery. 6th ed. Elsevier/Churchill Livingstone; 2011.
- Tan O, Atik B, Dogan A, Alpaslan S, Uslu M. Middle phalangectomy: a functional and aesthetic cure for macrodactyly. Scand J Plast Reconstr Surg Hand Surg. 2006;40(6):362-5. doi: 10.1080/02844310500369938. PMID: 17118902.
