
In this week's edition
- ✍️ Letter from P'Fella
The conference or the operating room? - 🤓 The Sunday Quiz
How well do you know Thumb MCPJ UCL injuries? - 🖼️ Image of the Week
The anatomy of a Seymour fracture. - 🚑 Technique Tip
An overview of the flexor teno washout procedure. - 👁️ What's Trending?
Google's Gemini 2.0 AI diagnoses pancreatitis from a CT. - 📋 Featured This Week
Plastics wrapped of 2024: In case you missed it! - 📖 What Does the Evidence Say
On reattaching ring avulsion injuries involving the PIPJ? - 🔥 Articles of the Week
Flexor tendon repairs, soft tissue defects of the hand, & hand burns management: with 1 sentence summaries. - 💕 Feedback
Suggest ideas & give feedback!
A Letter from P'Fella
Professor on Stage or Surgeon in Charge?
A recent tweet sparked a hot debate: Would you rather be the professor giving polished talks or the go-to surgeon trusted in critical moments? (See the original tweet here.)
Here’s the twist: Is this question really about the candidates — or does it reveal more about the biases baked into the way we define success in surgery? Let’s unpack it.
Let’s be real — patients care about results, not résumés. They want their surgeon to be the best in the OR, not the most sought-after speaker. Yet, without academics driving innovation, how would we advance as a field? The tension is clear: Is it more valuable to perfect a skillset or spread knowledge? And when these roles don’t overlap, who loses out?
Do A and B have to be mutually exclusive? Many surgeons combine technical mastery with academic leadership, proving a third option exists. This false dichotomy questions academics who rarely operate and technicians who don’t contribute to knowledge, but does it reveal more about the candidates — or our biases?
P'Fella ❤️
The Sunday Quiz
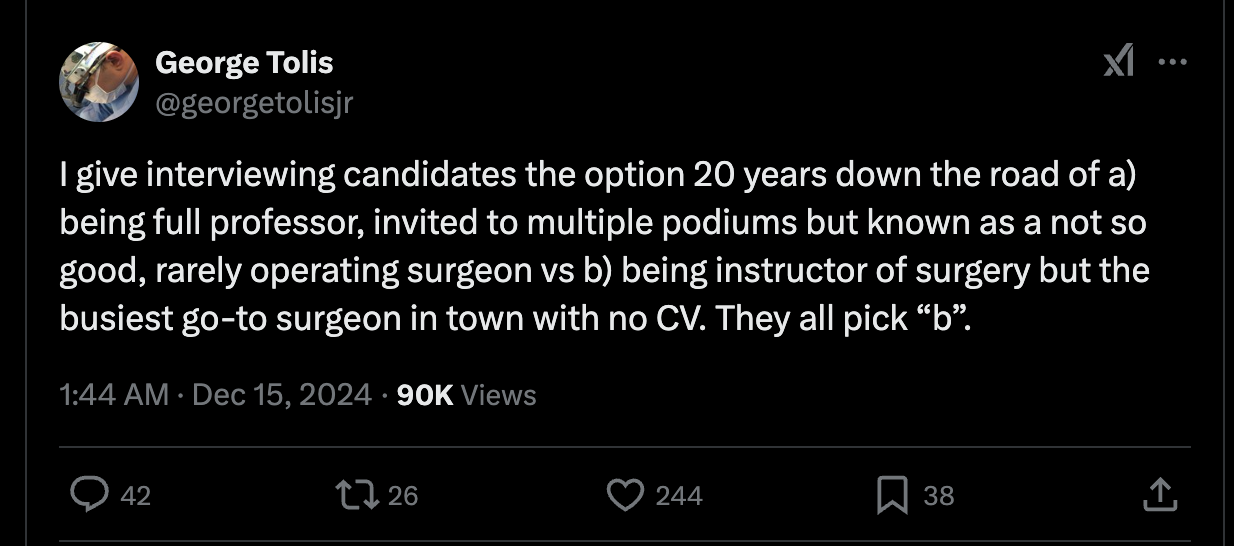
How Well Do You Know Thumb MCPJ UCL Injury?
Welcome to the next round of The Weekly Quiz.
Each edition of thePlasticsPaper includes a quiz question designed to challenge and engage our readers. Keep your wits about you and join in every week — the winner at the end of six rounds will earn you a one-year subscription to thePlasticsPro.
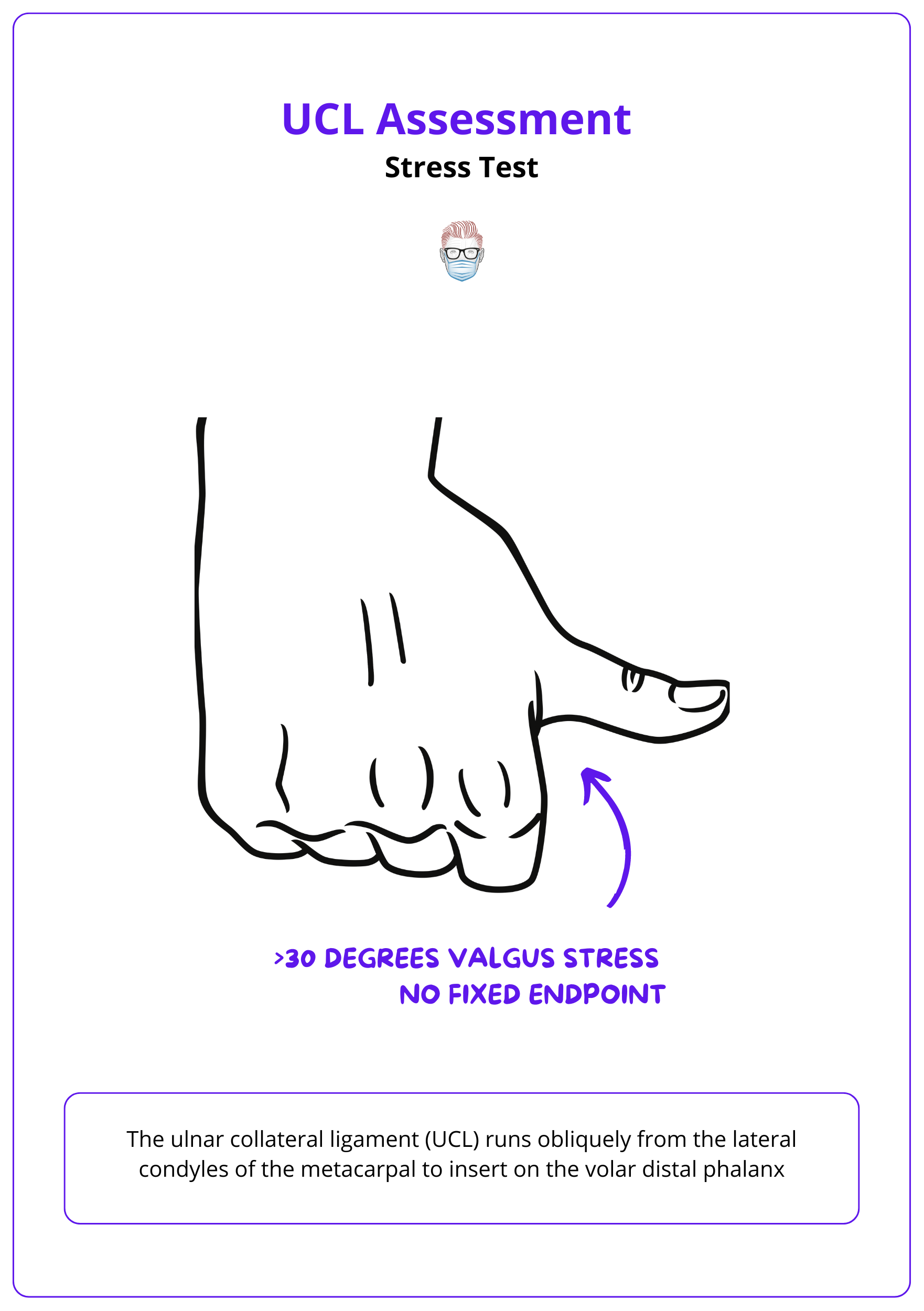
Image of the Week
Seymour Fracture Anatomy
In this section, we feature an anatomical illustration. This week, we’re looking at the anatomy of a Seymour fracture.
The injury presents as a pseudomallet, characterized by a flexion deformity of the distal phalanx, due to asymmetric tendon insertions.
Read more about Seymour fractures here.
Technique Tip
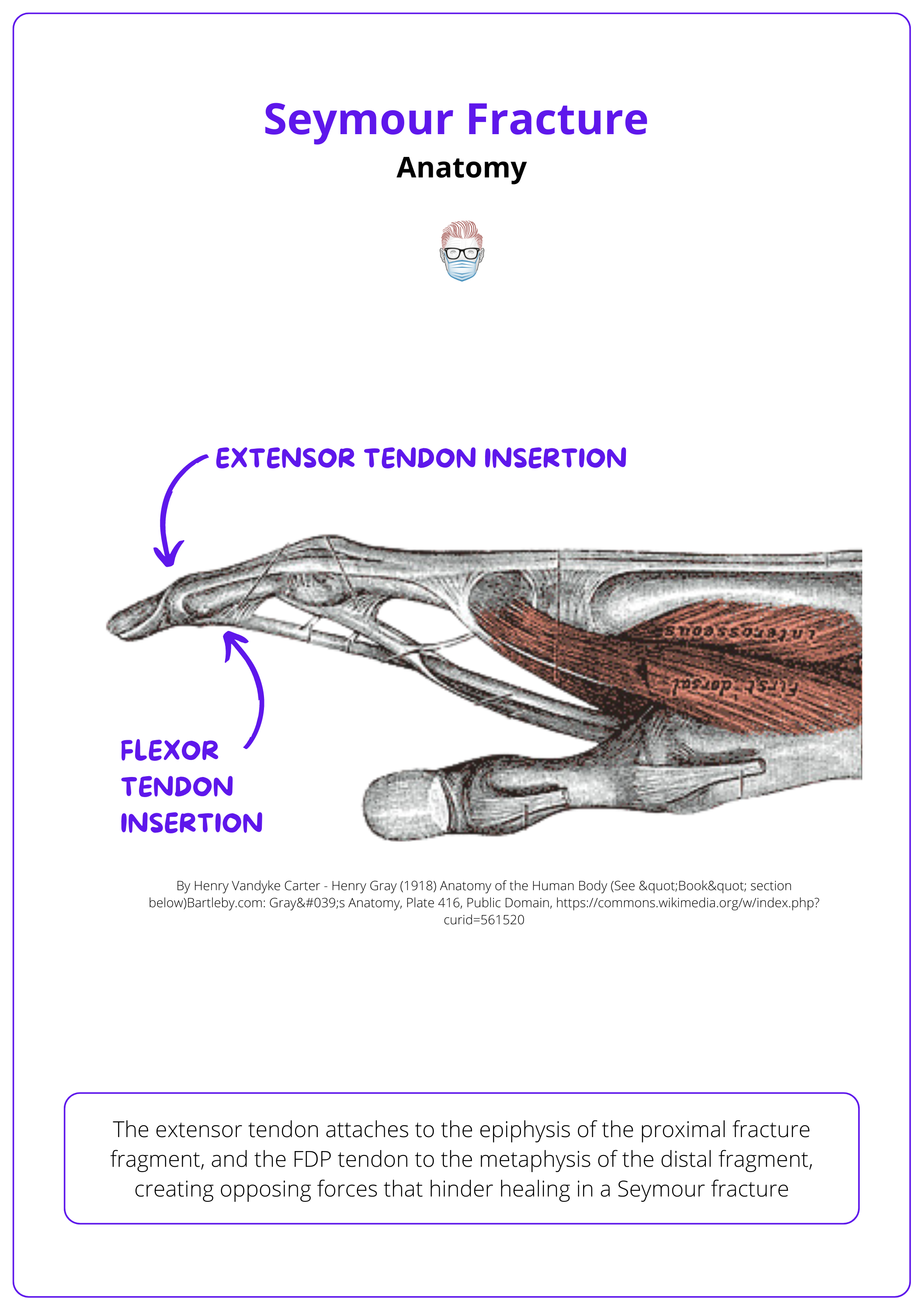
Flexor Teno Washout
This week’s technique focuses on flexor teno washout.
Flexor tenosynovitis washout involves limited incisions, such as a chevron at the A1 pulley, for targeted access and large-volume irrigation from proximal to distal. Severe cases may require carpal tunnel decompression and Parona space washout, especially in horseshoe abscesses. Intraoperative cultures guide antibiotic therapy, and the Michon Classification assesses severity.
Explore in more detail here.
What's Trending?
Gemini AI Diagnoses Pancreatitis from a CT
This edition looks at how Google's Gemini 2.0 AI diagnoses pancreatitis from a CT: A peek into the future of radiology.
From X, original source
Featured This Week
Plastics Wrapped of 2024
7 million minutes of learning across 190 countries. Discover the trends, top articles, and moments that shaped your year in plastic surgery with the Plastics Fella.
What Does the Evidence Say?
Should We Reattach Ring Avulsion Injuries Involving the PIPJ?
Extended debridement of the avulsed digital artery and the use of long venous grafts can enhance replantation success rates (Akyürek et al., 2002). However, replantation should be approached with caution in cases involving proximal phalanx fractures or flexor tendon lacerations, as these may result in significant mobility loss (Crosby et al., 2014). Long-term outcomes for complete ring avulsion amputations can be satisfactory in select patients (Adani et al., 2003).
Articles of the Week
3 Interesting Articles with 1 Sentence Summaries
Flexor tendon zone 2 repairs show high complication and reoperation rates; management emphasizes precise timing, surgical techniques, and tailored rehabilitation to optimize outcomes.
The reconstructive "elevator" approach for soft tissue defects of the hand; advanced pedicled, free fasciocutaneous, and venous flap options for functional and aesthetic success.
A roadmap for managing acutely burned hands: Precise burn depth assessment, multidisciplinary care, and strategies to preserve hand function and aesthetics while minimizing postburn contractures.
