

In this Article
Definition of Compartment Syndrome
Compartment syndrome is an increase in a pressure in a osseofascial compartment causing neurovascular compromise.
Pathophysiology
The pathophysiology of Compartment Syndrome is best described by Matsen’s Unified Hypothesis1. The Unified concept proposes that:
- The clinical features of compartment syndrome are the same, irrespective of etiology or location.
- Increased tissue pressure is the central pathogenic factor, which may be due to a decrease in compartment size or increase in the volume of its contents.
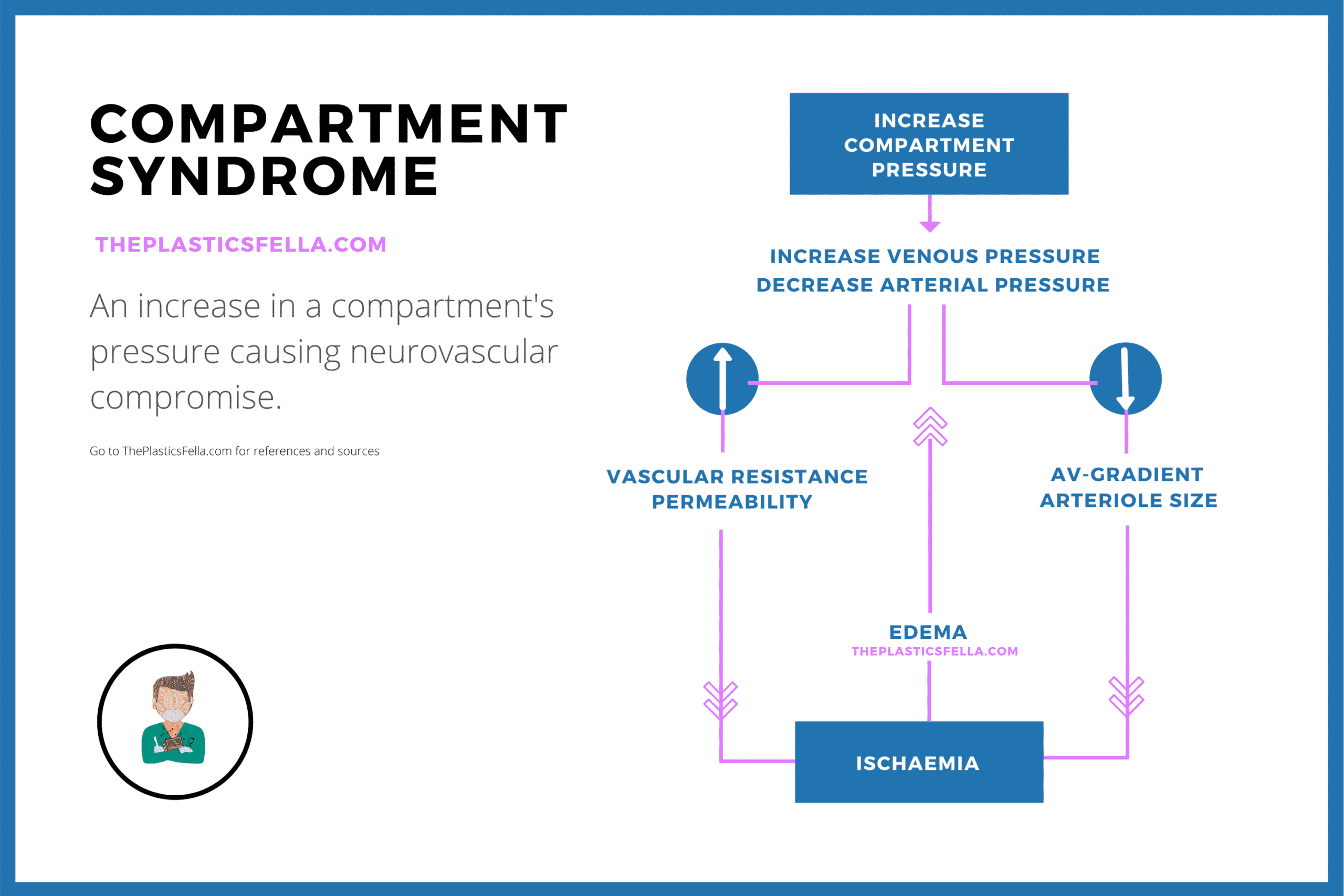
Current literature focuses on 3 pressure variables: interstitial tissue, venous pressure, arterial pressure. All of which are influenced by each-other in a positive-feedback loop. This feed-back loop creates the progressive nature of compartment syndrome and results in a spectrum of clinical findings, as illustrated in the diagram above1–5.
Stages of Compartment Syndrome
Compartment syndrome is a progressive clinical condition dependent on: the amount of pressurisation, duration of pressurisation and extent of soft tissue injury6. With these 3 factors in mind, a classification system has been proposed7
| Stage | Feature |
|---|---|
| Acute Incipient | – Early period after injury during – Pressures ≤ critical pressure |
| Acute Established-reversible | – Less than 8 hours – Urgent decompression avoids injury |
| Acute Established-irreversible | – More than 8 hours – Cellular death – Fasciotomy may still be useful |
| Late Established | – More than 8 hours – Prior to fibrous replacement of normal |
| Volkmann’s ischaemic contracture | – Fibrosis and contracture of affected compartment |
| Chronic exertional compartment syndrome | – Recurrent pressure increases – Transient symptoms – Usually during exercise & resolved with rest. |
Causes of Compartment Syndrome
Compartment syndrome can be caused by an increase in compartmental content or a decrease in compartmental size.
The aetiology of a compartment syndrome can be classified by the mechanism of the injury (traumatic vs non-traumatic) or the pathophysiology of the injury. Regardless of these classifications, injuries result in either an increase compartmental contents or decrease compartmental size.
The table outlines some of the causes of compartment syndrome:
| Common | Less Common |
|---|---|
| Fractures (e.g: carpometacarpal fracture-dislocation, distal radius or ulna, or a pediatric supracondylar humerus)7 | Muscle Overuse (e.g: Seziures) |
| Crush Injury | Infection (e.g: Abscess) |
| Burns8 | Bite9 |
| Bleeding10,11 | Nephrotic Syndrome |
| High-pressure injury12 | Reperfusion Injury13–15 |
| Constrictive banadages16 |
Diagnosis of Compartment Syndrome
Compartment syndrome is a clinical diagnosis, which may be assisted by compartment pressure readings.
Clinical Diagnosis
The diagnosis of compartment syndrome has traditionally focused on the 5P’s mnemonic:
- Pain
- Pallor
- Paraesthesia
- Paralysis
- Pulselessness.
The diagnostic sensitivity and specificity of the signs and symptoms are such that they cannot be used in isolation to make the diagnosis of an acute compartment syndrome.
This table summaries current evidence for clinical signs of compartment syndrome.
| Sign | Evidence |
|---|---|
| Pain | – Disproportionate to physical findings – Exacerbated by passive stretching – Peaks at 2-6 hours of ischemia and then subsides with necrosis – The most reliable sign7,17 |
| Pallor | – Less reliable – Can have good skin colour overlying a pressurised compartment18 due to way blood is supplied to skin. |
| Pressure | – Tense, swollen compartment17 – Intrinsic minus position |
| Paraesthesia | – Progressive neurologic changes19 – Can be confounded by injury |
| Late Signs | Paralysis and pulselessness are late signs. Irreversible tissue damage can occur in the presence of palpable pulse – the critical compartment pressure is capillary filling pressure, which is lower than arterial pressure20. |
In a paediatric population, the rule of “A’s” has been suggested: analgesia, anxiety, agitation
Pressure Measurements
There is an ongoing debate regarding the role of interstitial pressure measurements. There is a general consensus on their accuracy if performed correctly, but differing opinions on its utility.
Indications include an unresponsive patient, polytrauma, inconclusive clinical examination. Limitations of interstitial pressure measurements include:
- Differences in pressure depending on location of measurement21
- Fracture-related injuries can cause high pressures than other types of injuries22
- Several different techniques, with no convincing superiority study23–26
Newer techniques have been described to overcome these limitations:
- Laser Doppler flowmetry27
- 99Tcm-methoxy-isobutryl isonitril scintigraphy28
Pressure Values
There is no exact pressure value to diagnose compartment syndrome. On reviewing the literature, there appears to be 3 schools of thought for diagnosis:
- Absolute interstitial pressure between 30-50mmHg25,29,30
- Delta Pressure ≤ 30mmgHg (difference between the diastolic blood pressure and the compartment pressure)31,32
- Interstitial tissue pressures within 30 mmHg of the mean arterial pressure or 20 mmHg of the diastolic blood pressure33
On a physiological level, the following numbers are important:
- Normal interstitial fluid pressures between 0 and 25.2 mm Hg34,35
- Axonal transport slows with a pressure of 30mmHg36
- Arteriole collapse occurs at 30-40mmHg2
- Motor and sesonry conduction stops at 50mmHg37.
Initial Management of Compartment Syndrome
Early recognition and high index of suspicion is vital to minimize tissue necrosis and functional loss. Initial management can often be done at the bedside whilst awaiting theatre.
At the Bedside
- Remove all constrictive dressings
- Elevation of the limb to heart level38
- Frequent clinical assessments
- Consider Pressure Measurements
Medical Optimisation
- Knowledge and optimisation of comorbidities
- Fluid and electrolyte management
- Monitoring of renal function and for signs of coagulopathy are important.
- Urinalysis for myoglobinuria
- Elevated levels of serum creatinine phosphokinase may indicate severe muscle damage.
Radiological Investigations
This is a case-by-case basis guided by history and clinical examination. Post-decompression, there are case reports describing the use of MRI to assess degree of myonecrosis 39
Surgical Fasciotomy of the Hand
Urgent surgical decompression through well-planned fasciotomy incisions is the surgical management for compartment syndrome.
The hand has 10 separate compartments. It is rarely necessary to release all 10 compartments, and intraoperative assessment and/or measurement of compartment pressures should be used to determine the extent of release needed. If possible, pre-operatively consent patient in relation to scars
Compartments of the Hands and the Incision
The following table describe the compartment, muscles and their respective incisions for decompression.
For more information on flexor tendon anatomy, click here.
| Compartment | Muscles | Fasciotomy Incision |
|---|---|---|
| Hypothenar | Abductor digiti minimi Flexor digiti minimi Opponens digiti minimi | Ulnar border of hand |
| Thenar | Abductor pollicis brevis Oponens pollicis Flexor pollicis brevis | Radial margin of thenar eminence |
| Adductor Pollicis | Two Heads | Dorsal over first webspace |
| Dorsal Interosseous | 4 compartments40 | Between 2-3rd & 4-5th metacarpals. |
| Volar Interosseous | 3 compartments41 | Extended carpal tunnel incision |
3 Volar Fasciotomy Incisions
Incision 1: Extended carpal tunnel incision
The aim of this incision is to release:
- Ulnar Neurovascular structures: release of Guyon’s Canal
- Adductor Pollicis: extend incision into second volar web space.
- Volar Interosseous Muscle: separate fascia between middle finger metacarpal and palmar fascia
Incision 2 and 3: Radial and Ulnar Incisions
- The thenar muscles are released via a longitudinal incision on radial margin of thenar eminence
- The hypothenar muscles are released via a longitudinal incision on ulnar border of the hand.
3 Dorsal Fasciotomy Incisions
Incision 1: Longitudinal Incision in 1st Webspace
- First dorsal interosseous muscle – incision in first webspace (can also release the dorsal fascia of the adductor pollicis)
Incision 2 & 3: Longitudinal Incision in 2nd-3rd, 4-5th Metacarpal spacepace
- Remaining dorsal interosseous muscles – incision between 2nd-3rd, 4th-5th metacarpals (can also decompression volar interosseus muscles)
Release of Fingers
Dermotomies are not always indicated but should be performed if tense & swollen fingers The tight fibers of Cleland and Grayson ligaments can compression and obstruct the Digital arteries. These ligaments compartmentalise the digits.
Ideally, a dermotomy should be a mid-axial incision (ulnar for index, long and ring, radial for thumb and little finger).
Post-Operatively
In the post-operative setting for hand fasciotomies, key principles are:
- Limb should be splinted in a position of function and elevated with avoidance of constrictive dressings.
- Careful monitoring of adjacent compartments for emerging pathology
- Re-evaluate the wound every 24-48 hours
- Debridement of all nonviable tissue
- Consider use of Negative-pressure wound therapy
- Optimisation medically and control pain
- Therapy should be started immediately promote maximum range of movement
References
- 1. Matsen F. Compartmental syndrome. An unified concept. Clin Orthop Relat Res. 1975;(113):8-14. https://www.ncbi.nlm.nih.gov/pubmed/1192678
- 2. ASHTON H. Critical closing pressure in human peripheral vascular beds. Clin Sci. 1962;22:79-87. https://www.ncbi.nlm.nih.gov/pubmed/13862865
- 3. BURTON A. On the physical equilibrium of small blood vessels. Am J Physiol. 1951;164(2):319-329. doi:10.1152/ajplegacy.1951.164.2.319
- 4. BENJAMIN A. The relief of traumatic arterial spasm in threatened Volkmann’s ischaemic contracture. J Bone Joint Surg Br. 1957;39-B(4):711-713. https://www.ncbi.nlm.nih.gov/pubmed/13491634
- 5. Hargens A, Mubarak S. Current concepts in the pathophysiology, evaluation, and diagnosis of compartment syndrome. Hand Clin. 1998;14(3):371-383. https://www.ncbi.nlm.nih.gov/pubmed/9742417
- 6. Matava MJ, Whitesides TE Jr, Seiler JG III, Hewan-Lowe K, Hutton WC. DETERMINATION OF THE COMPARTMENT PRESSURE THRESHOLD OF MUSCLE ISCHEMIA IN A CANINE MODEL. The Journal of Trauma: Injury, Infection, and Critical Care. Published online July 1994:50-58. doi:10.1097/00005373-199407000-00010
- 7. Leversedge FJ, Moore TJ, Peterson BC, Seiler JG III. Compartment Syndrome of the Upper Extremity. The Journal of Hand Surgery. Published online March 2011:544-559. doi:10.1016/j.jhsa.2010.12.008
- 8. Mann R, Wallquist J. Early decompression fasciotomy in the treatment of high-voltage electrical burns of the extremities. South Med J. 1975;68(9):1103-1108. doi:10.1097/00007611-197509000-00012
- 9. Brys AK, Gandolfi BM, Levinson H, Gerardo CJ. Copperhead Envenomation Resulting in a Rare Case of Hand Compartment Syndrome and Subsequent Fasciotomy. Plastic and Reconstructive Surgery – Global Open. Published online May 2015:e396. doi:10.1097/gox.0000000000000367
- 10. Kim J, Buck D, Forte A, et al. Risk factors for compartment syndrome in traumatic brachial artery injuries: an institutional experience in 139 patients. J Trauma. 2009;67(6):1339-1344. doi:10.1097/TA.0b013e318197b999
- 11. Hay SM, Allen MJ, Barnes MR. Acute compartment syndromes resulting from anticoagulant treatment. BMJ. Published online December 12, 1992:1474-1475. doi:10.1136/bmj.305.6867.1474
- 12. Vidal R, Kissoon N, Gayle M. Compartment syndrome following intraosseous infusion. Pediatrics. 1993;91(6):1201-1202. https://www.ncbi.nlm.nih.gov/pubmed/8502531
- 13. Seiler JG III, Olvey SP. Compartment syndromes of the hand and forearm. Journal of the American Society for Surgery of the Hand. Published online November 2003:184-198. doi:10.1016/s1531-0914(03)00072-x
- 14. Grace P. Ischaemia-reperfusion injury. Br J Surg. 1994;81(5):637-647. doi:10.1002/bjs.1800810504
- 15. Jensen S, Sandermann J. Compartment syndrome and fasciotomy in vascular surgery. A review of 57 cases. Eur J Vasc Endovasc Surg. 1997;13(1):48-53. doi:10.1016/s1078-5884(97)80050-0
- 16. Ashton H. Effect of inflatable plastic splints on blood flow. BMJ. Published online December 10, 1966:1427-1430. doi:10.1136/bmj.2.5527.1427
- 17. Gelberman R, Garfin S, Hergenroeder P, Mubarak S, Menon J. Compartment syndromes of the forearm: diagnosis and treatment. Clin Orthop Relat Res. 1981;(161):252-261. https://www.ncbi.nlm.nih.gov/pubmed/7307388
- 18. Whitesides T, Heckman M. Acute Compartment Syndrome: Update on Diagnosis and Treatment. J Am Acad Orthop Surg. 1996;4(4):209-218. doi:10.5435/00124635-199607000-00005
- 19. Szabo R, Gelberman R. Peripheral nerve compression: etiology, critical pressure threshold, and clinical assessment. Orthopedics. 1984;7(9):1461-1466. doi:10.3928/0147-7447-19840901-11
- 20. Mubarak S, Owen C. Double-incision fasciotomy of the leg for decompression in compartment syndromes. J Bone Joint Surg Am. 1977;59(2):184-187. https://www.ncbi.nlm.nih.gov/pubmed/15455478
- 21. Seiler J, Womack S, De L, Whitesides T, Hutton W. Intracompartmental pressure measurements in the normal forearm. J Orthop Trauma. 1993;7(5):414-416. doi:10.1097/00005131-199310000-00003
- 22. Heckman M, Whitesides T, Grewe S, Rooks M. Compartment pressure in association with closed tibial fractures. The relationship between tissue pressure, compartment, and the distance from the site of the fracture. J Bone Joint Surg Am. 1994;76(9):1285-1292. doi:10.2106/00004623-199409000-00002
- 23. Reneman R. The anterior and the lateral compartmental syndrome of the leg due to intensive use of muscles. Clin Orthop Relat Res. 1975;(113):69-80. doi:10.1097/00003086-197511000-00011
- 24. Rorabeck C, Castle G, Hardie R, Logan J. Compartmental pressure measurements: an experimental investigation using the slit catheter. J Trauma. 1981;21(6):446-449. https://www.ncbi.nlm.nih.gov/pubmed/7230297
- 25. Matsen F, Mayo K, Sheridan G, Krugmire R. Monitoring of intramuscular pressure. Surgery. 1976;79(6):702-709. https://www.ncbi.nlm.nih.gov/pubmed/1273755
- 26. Barnes MR, Gibson MJ, Scott J, Bentley S, Allen MJ. A technique for the long term measurement of intra-compartmental pressure in the lower leg. Journal of Biomedical Engineering. Published online January 1985:35-39. doi:10.1016/0141-5425(85)90006-8
- 27. Abraham P, Leftheriotis G, Saumet J. Laser Doppler flowmetry in the diagnosis of chronic compartment syndrome. J Bone Joint Surg Br. 1998;80(2):365-369. doi:10.1302/0301-620x.80b2.7963
- 28. Edwards P, Miles K, Owens S, Kemp P, Jenner J. A new non-invasive test for the detection of compartment syndromes. Nucl Med Commun. 1999;20(3):215-218. doi:10.1097/00006231-199903000-00003
- 29. Dahn I, Lassen N, Westling H. Blood flow in human muscles during external pressure or venous stasis. Clin Sci. 1967;32(3):467-473. https://www.ncbi.nlm.nih.gov/pubmed/6028126
- 30. Matsen F, Mayo K, Krugmire R, Sheridan G, Kraft G. A model compartmental syndrome in man with particular reference to the quantification of nerve function. J Bone Joint Surg Am. 1977;59(5):648-653. https://www.ncbi.nlm.nih.gov/pubmed/141451
- 31. McQueen M, Gaston P, Court-Brown C. Acute compartment syndrome. Who is at risk? J Bone Joint Surg Br. 2000;82(2):200-203. doi:10.1302/0301-620x.82b2 .9799
- 32. Matsen F, Krugmire R. Compartmental syndromes. Surg Gynecol Obstet. 1978;147(6):943-949. https://www.ncbi.nlm.nih.gov/pubmed/362581
- 33. Whitesides T, Haney T, Harada H, Holmes H, Morimoto K. A simple method for tissue pressure determination. Arch Surg. 1975;110(11):1311-1313. doi:10.1001/archsurg.1975.01360170051006
- 34. Zandi H. Results of compartment decompression in chronic forearm compartment syndrome: six case presentations. British Journal of Sports Medicine. Published online September 1, 2005:e35-e35. doi:10.1136/bjsm.2004.012518
- 35. Ardolino A, Zeineh N, O’Connor D. Experimental Study of Forearm Compartmental Pressures. The Journal of Hand Surgery. Published online October 2010:1620-1625. doi:10.1016/j.jhsa.2010.06.017
- 36. Dahlin LB, Rydevik B, McLean WG, Sjöstrand J. Changes in fast axonal transport during experimental nerve compression at low pressures. Experimental Neurology. Published online April 1984:29-36. doi:10.1016/0014-4886(84)90003-7
- 37. Hargens AR, Botte MJ, Swenson MR, Gelberman RH, Rhoades CE, Akeson WH. Effects of local compression on peroneal nerve function in humans. J Orthop Res. Published online November 1993:818-827. doi:10.1002/jor.1100110607
- 38. Chidgey L, Szabo R, Kolack B. Effects of elevation on nerve function in an acute upper extremity nerve compression model. J Orthop Res. 1989;7(6):783-791. doi:10.1002/jor.1100070603
- 39. Mehta V, Chowdhary V, Lin C, Jbara M, Hanna S. Compartment syndrome of the hand: A case report and review of literature. Radiology Case Reports. Published online February 2018:212-215. doi:10.1016/j.radcr.2017.11.002
- 40. Halpern A, Mochizuki R, Long C. Compartment syndrome of the forearm following radial-artery puncture in a patient treated with anticoagulants. J Bone Joint Surg Am. 1978;60(8):1136-1137. https://www.ncbi.nlm.nih.gov/pubmed/721868
- 41. DiFelice A, Seiler J, Whitesides T. The compartments of the hand: an anatomic study. J Hand Surg Am. 1998;23(4):682-686. doi:10.1016/S0363-5023(98)80055-5
