
In this week's edition
- ✍️ Letter from P'Fella
Plastic surgery’s biggest lie? Its own literature - 🤓 The Sunday Quiz
How well do you know median nerve tendon transfers? - 🖼️ Image of the Week
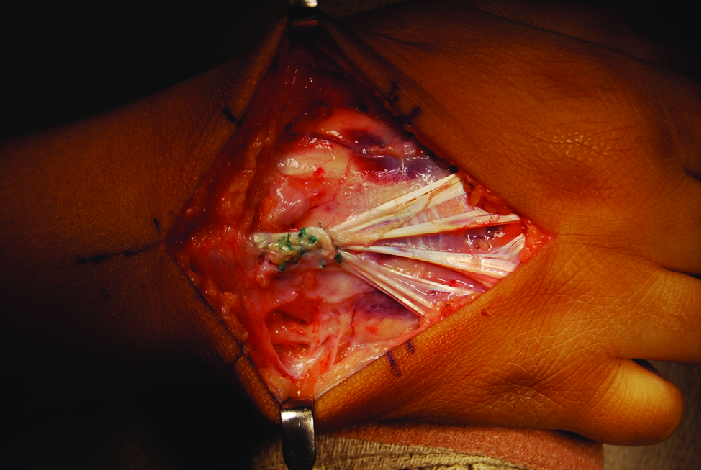
Intraoperative picture of an extensor tendon transfer. - 🚑 Technique Tip
Pulvertaft weave technique - 📙 Foundations Textbook
Progress update: February - 📖 What Does the Evidence Say
How many pulleys should we save? - 🔥 Articles of the Week
Flexor tendon injuries in 2024, partial extensor tendon injuries, & tendon transfer review: with 1 sentence summaries. - 💕 Feedback
Suggest ideas & give feedback!
A Letter from P'Fella
Plastic Surgery’s Biggest Lie? Its Own Literature
Here’s the uncomfortable truth: a huge chunk of plastic surgery literature is wrong, yet we keep citing it like gospel.
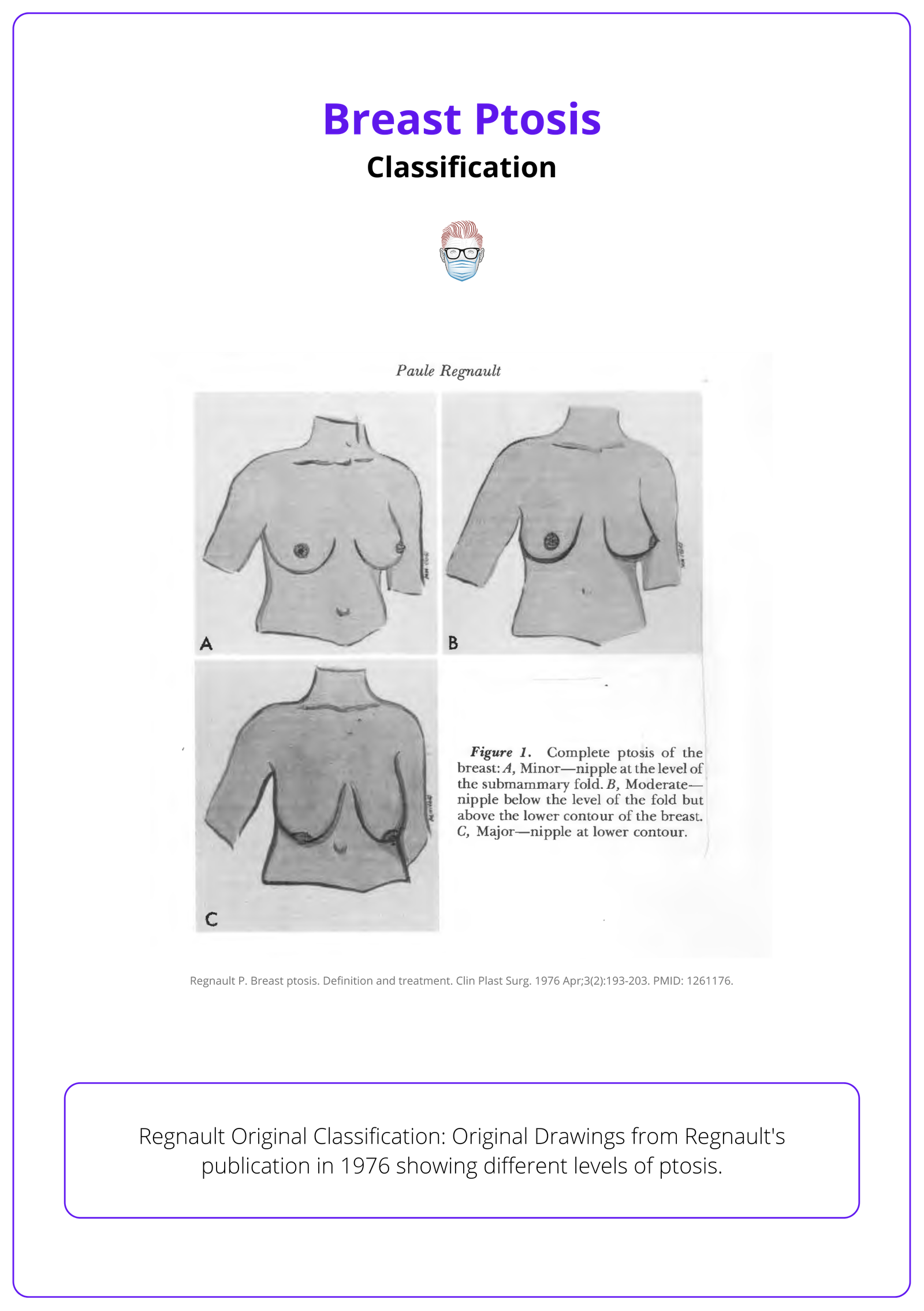
Take breast ptosis. Regnault’s 1976 classification was simple — three types and pseudoptosis. But today? Some papers claim five classifications, others tweak definitions, and suddenly, the field can’t even agree on a basic concept.
Why? Because nobody reads the original research.
The Broken Game of Academic Telephone
Regnault’s paper is paywalled, so instead of verifying the source, researchers copy from the last paper — errors and all. Over time, minor mistakes become accepted facts. The result?
- Textbooks are full of misinformation: What’s taught today isn’t what was originally described.
- Systematic reviews are reinforcing bad data: If the foundation is wrong, the conclusions are useless.
- Clinical decisions are based on a flawed understanding: If we can’t even classify ptosis correctly, what else are we getting wrong?
This isn’t just about breast ptosis — it’s happening across plastic surgery.
How Did We Let This Happen?
Plastic surgery prides itself on being evidence-based — but what happens when the evidence itself is broken?
We’ve built a system that rewards repetition over verification. Instead of going back to original sources, we trust whatever the last paper says. Paywalls keep key research locked away, so errors go unchallenged. And once misinformation makes it into a textbook or systematic review, it becomes fact — not because it’s true, but because it’s been repeated enough times.
The fix?
- Stop trusting secondhand sources. If a paper cites something, pull the original.
- If an article gets it wrong, call it out — silence allows bad information to spread.
- And if we actually care about advancing the field, we need to push for open access — because what good is knowledge if nobody can verify it?
With love,
P'Fella ❤️
The Sunday Quiz
How Well Do You Know Median Nerve Tendon Transfers?
Welcome to the next round of The Weekly Quiz.
Each edition of thePlasticsPaper includes a quiz question designed to challenge and engage our readers. Keep your wits about you and join in every week — the winner at the end of six rounds will earn you a one-year subscription to thePlasticsPro.
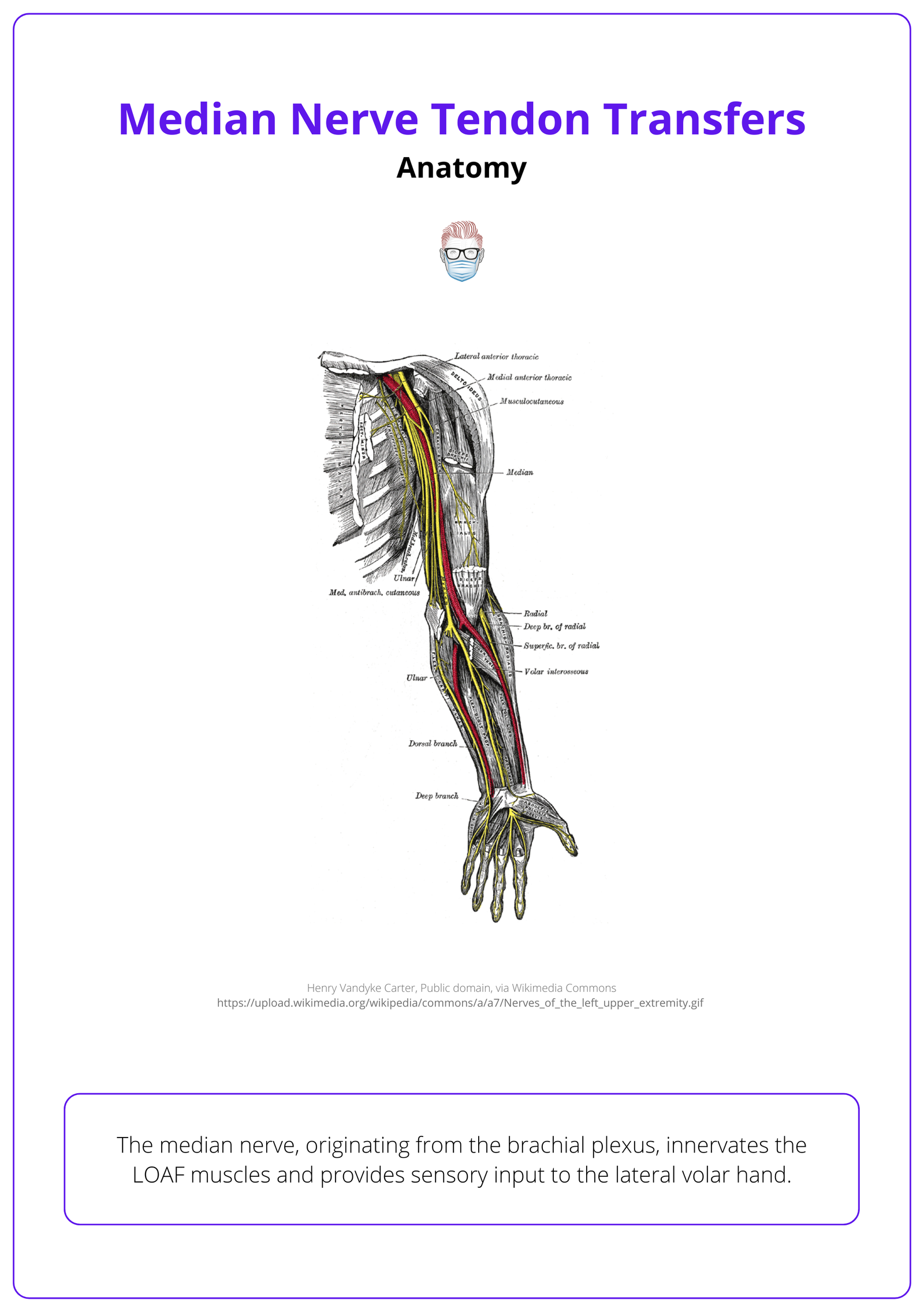
Image of the Week
Extensor Tendon Transfer
In this section, we feature an anatomical illustration. This week, we’re looking at an intraoperative picture demonstrating the extensor carpi radialis longus (ECRL) sutured to the extensor digitorum communis using a Pulvertaft weave.
Digital extensor hypoplasia (DEH) is a rare malformation that presents with loss of active finger extension at the metacarpophalangeal (MCP) joints.
Technique Tip
Pulvertaft Weave
This week’s technique focuses on Pulvertaft Weave, a fundamental method in tendon transfer surgeries. This technique involves interlacing the donor tendon into the recipient tendon to ensure a secure and durable connection.
For a visual demonstration, below is Dr. Badia's explanation of the Pulvertaft Weave technique.
Foundations Textbook
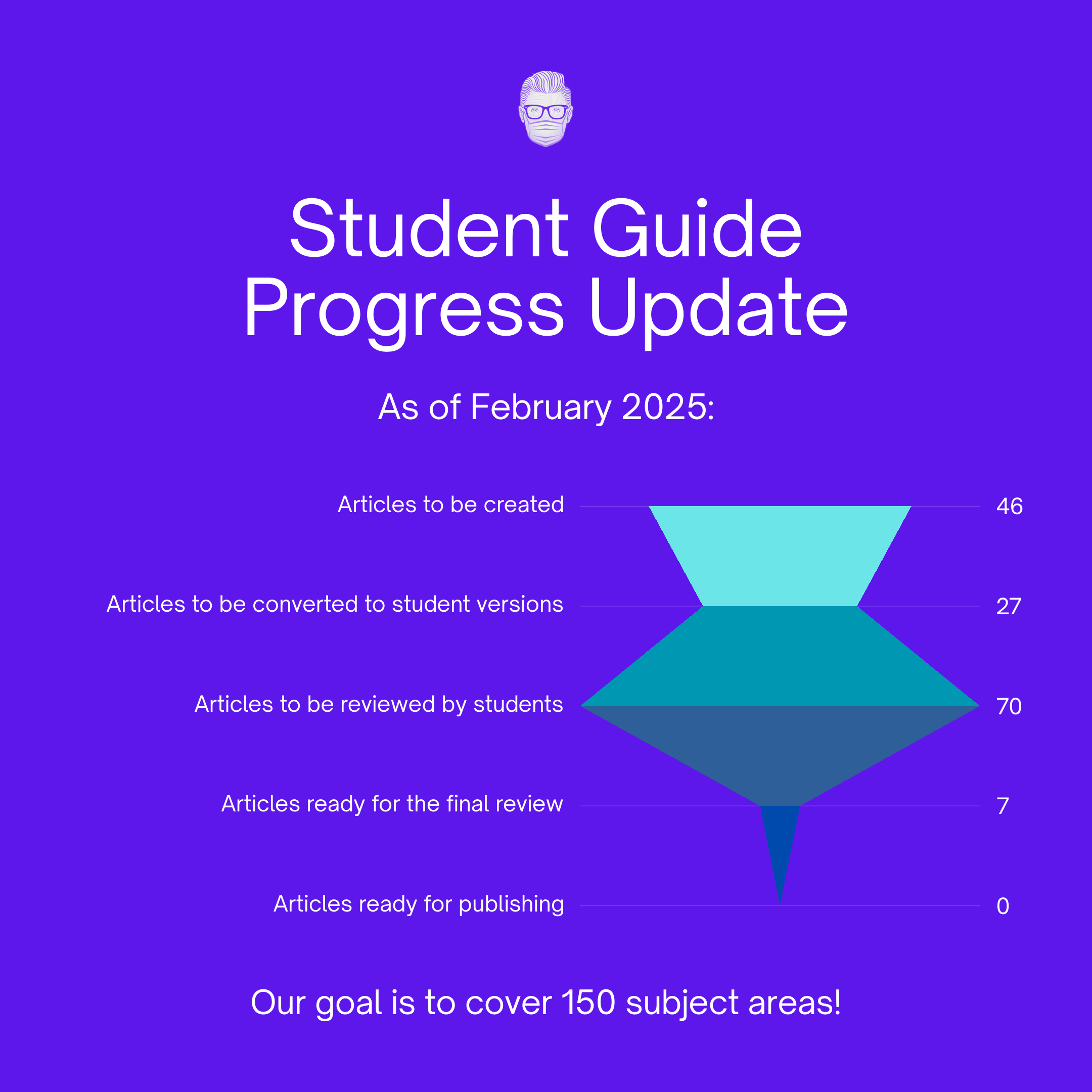
February Update
In line with our "Building in Public" approach, we’re keeping you in the loop on the latest developments in the Plastic Surgery Student Guide.
What Does the Evidence Say?
How Many Pulleys Should We Save?
Various techniques for pulley management during repair have been described, including venting, plasty, and complete release (Goubier et al., 2014; Bunata, 2010; Pan et al., 2017). Strong core suture techniques, such as the 6-strand M-Tang method, allow for early active motion protocols without peripheral sutures (Giesen et al., 2018).
Biomechanical studies have shown that intact pulleys can decrease repair strength (Cao & Tang, 2009). Overall, judicious pulley release during flexor tendon repair appears to be safe and may improve outcomes by allowing better tendon gliding and reducing the risk of repair rupture (Zafonte et al., 2014; Pan et al., 2017; Giesen et al., 2018).
Articles of the Week
3 Interesting Articles with 1 Sentence Summaries
Flexor tendon injuries pose high complication risks, especially in zone 2, requiring careful timing, technique, and soft tissue management for optimal outcomes.
Non-operative management of selected partial extensor tendon lacerations is safe, with comparable grip strength and return-to-work times to surgical repair, but higher complication rates in repaired cases.
Nerve transfers are increasingly favored for peripheral nerve injuries, often combined with tendon transfers to optimize function while preserving reconstruction options.
