

Summary Card
Definition
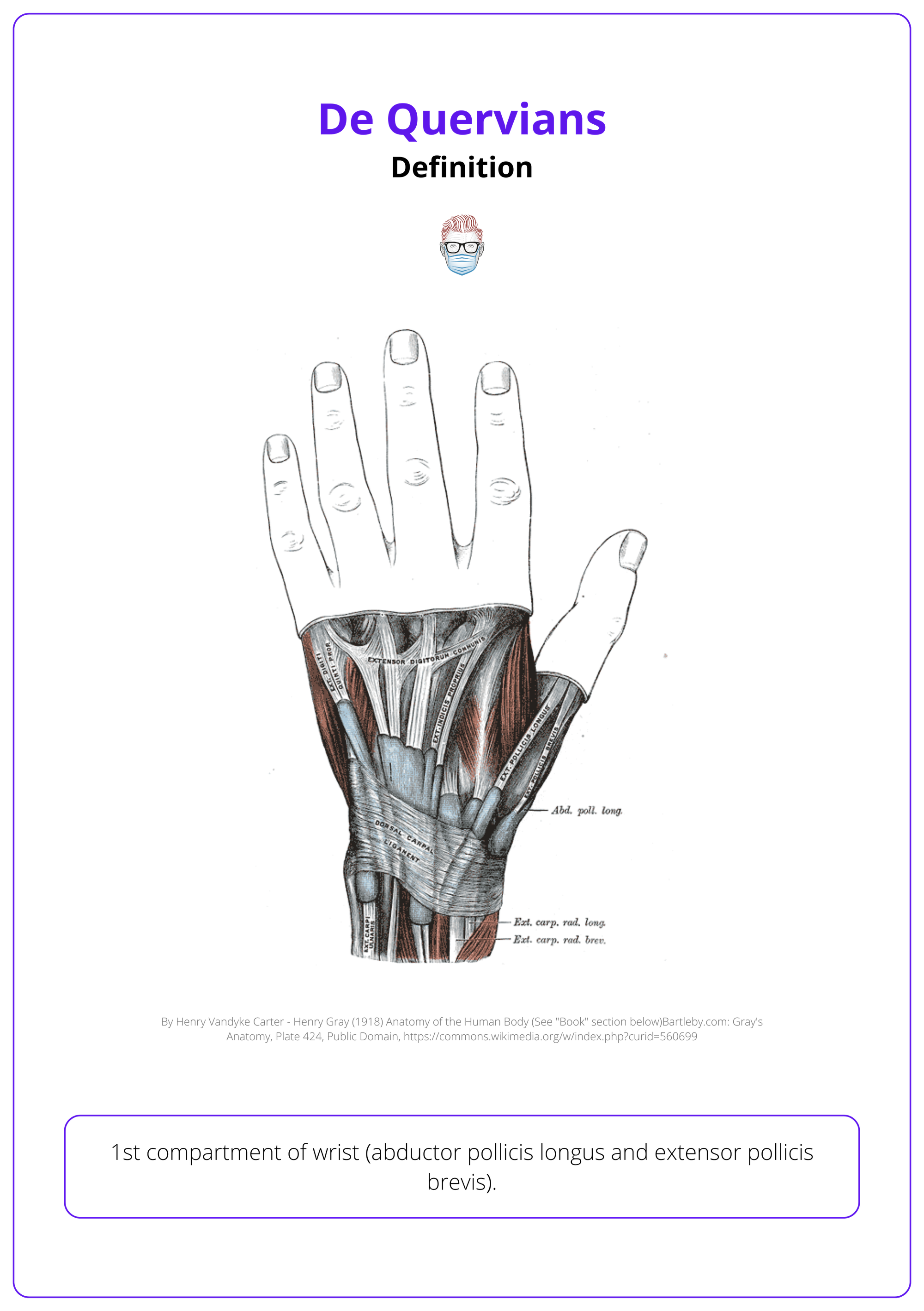
de Quervain disease, also known as stenosing tenosynovitis, affects the first dorsal compartment of the wrist.
Clinical Features
Presents with pain that is worsened by grasping, thumb abduction, and radial and ulnar deviation of the wrist.
Investigations
Diagnosis is primarily clinical, using provocative tests such as Finkelstein and Eichoff.
Treatment
First line treatment is conservative. Surgical release of the first write compartment can be done if conservative measures are not successful.
Primary Contributor: Dr Waruguru Wanjau, Educational Fellow.
Reviewer: Dr Suzanne Thomson, Educational Fellow.
Definition of De Quervians
de Quervain disease, also known as stenosing tenosynovitis, affects the first dorsal compartment of the wrist, often seen in individuals with repetitive wrist movements or during pregnancy and postpartum.
de Quervain's disease involves entrapment of the APL and EPB tendons in the first dorsal compartment due to inflammatory, attritional, and degenerative changes.
- Repetitive Movements: Repeated thumb abduction, extension, and radial deviation increase stress on the tendons.
- Pathological Changes: Thickened tendon sheaths compress the compartment, causing stenosing tenosynovitis. Fibrocartilage formation and myxoid degeneration further contribute to the condition.
- Systemic Factors: Systemic inflammatory conditions like rheumatoid arthritis can sometimes exacerbate the pathology.
It is also known as stenosing tendinitis, peritendinitis, styloid tenovaginitis, and stenosing tendovaginitis.
The condition often affects women, particularly in late pregnancy or the postpartum period, due to specific repetitive movements and hormonal changes (Shuaib, 2014). Other risk factors include:
- Manual labor
- Repetitive wrist movements
- Activities requiring thumb stabilization (Ilyas, 2007)
Anatomical variations, such as septation in the first dorsal compartment, occur in 60% of symptomatic cases, while multiple APL tendons are present in 76% of patients.
Clinical Features of De Quervians
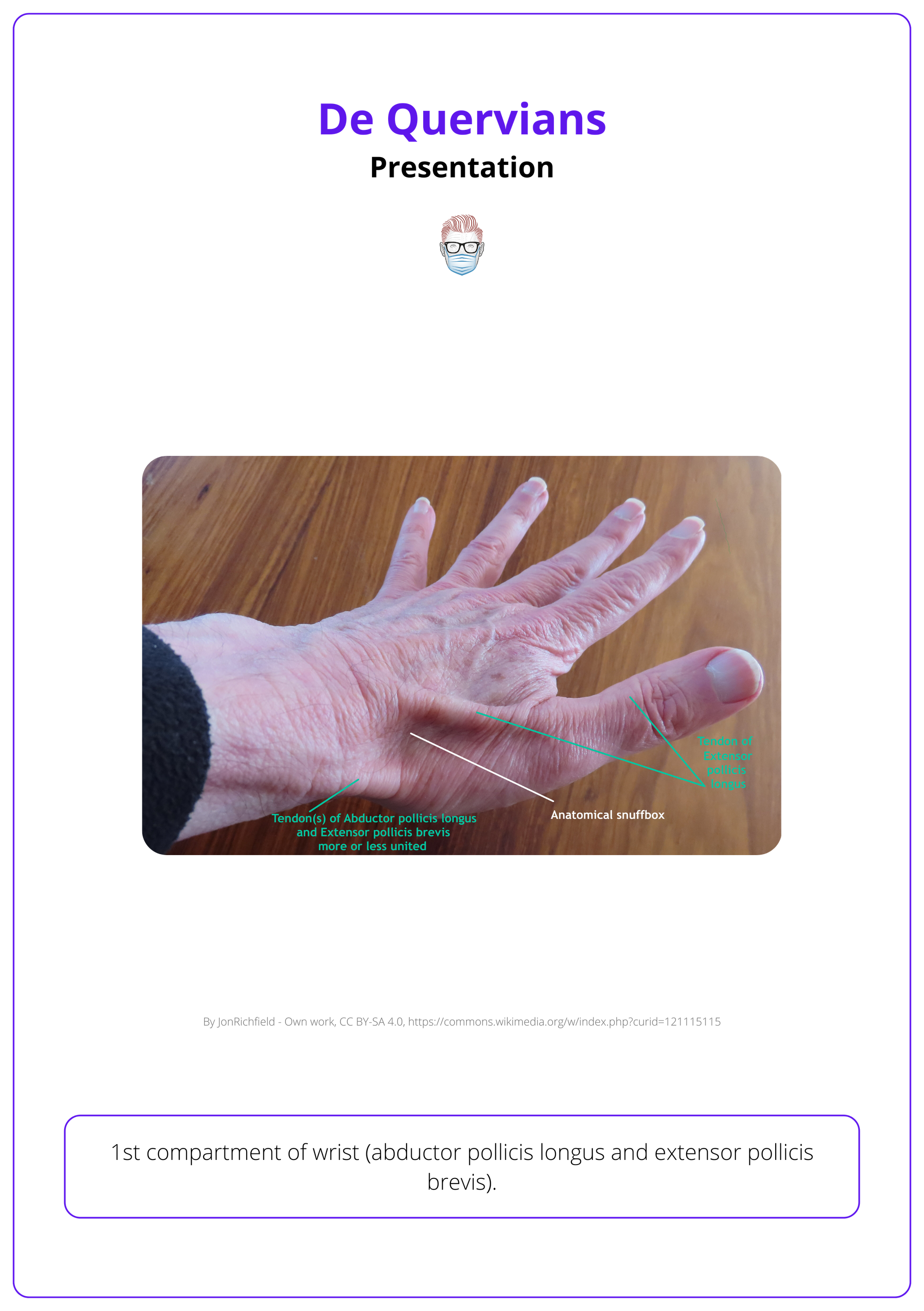
de Quervain's disease presents with pain that is worsened by activities like grasping, thumb abduction, and radial or ulnar deviation of the wrist.
History
- Pain and tenderness localized to the radial styloid area.
- Pain worsens with activities such as thumb abduction, grasping, and wrist deviation.
- Bilateral involvement is common, especially in new mothers or caregivers.
- Rare symptoms may include thumb triggering, locking, or development of a dorsal ganglion cyst.
Examination
- Swelling may be present proximal to the radial styloid.
- Tenderness along the first dorsal compartment.
- WHAT Test: Wrist hyperflexion and thumb abduction to provoke symptoms and confirm de Quervain's diagnosis.
- Finkelstein Test and Eichoff Test: Highly sensitive for de Quervain’s tenosynovitis, aiming to reproduce sharp pain along the radial wrist.

Differential Diagnosis for Radial-Sided Wrist Pain
Differentiating de Quervain's from thumb CMC osteoarthritis is critical. In de Quervain's, pain is typically localized to the first dorsal compartment, while CMC arthritis involves the base of the thumb.
- Thumb Carpometacarpal Joint Osteoarthritis: Typically presents with pain at the base of the thumb and crepitus on movement.
- Intersection Syndrome: Pain is usually located more proximal to the radial styloid, with crepitus during wrist extension and radial deviation.
- Wartenberg Syndrome: Involves compression of the superficial radial nerve, presenting with pain and paresthesia along the dorsum of the thumb.
Histopathology of de Quervain's disease typically shows no inflammation, but instead thickening of the extensor tendons and the surrounding retinaculum (Ilyas, 2007).
Extensor triggering or locking of the thumb, as well as dorsal ganglion cyst formation, are rare but recognized presentations of de Quervain's disease. (Ilyas 2007)
Investigations for De Quervains
Diagnosis is clinical: X-ray rules out fractures, ultrasound identifies septation, and MRI is for atypical cases.
- X-Ray: Useful to rule out other causes of radial wrist pain, such as thumb CMC joint osteoarthritis or fractures.
- Ultrasound: Highly effective for identifying septation in the first dorsal compartment, crucial for surgical planning to ensure a comprehensive release. Doppler ultrasound may help assess dynamic changes during wrist movement.
- MRI: Reserved for atypical cases to assess for alternative diagnoses, including soft tissue tumors or other tenosynovitis.
Ultrasound is helpful for identifying septation in the first dorsal compartment to ensure complete release.
Anatomical variations, such as septation or multiple APL tendons, are common in de Quervain's and can affect both non-operative and surgical management
Treatment of De Quervains
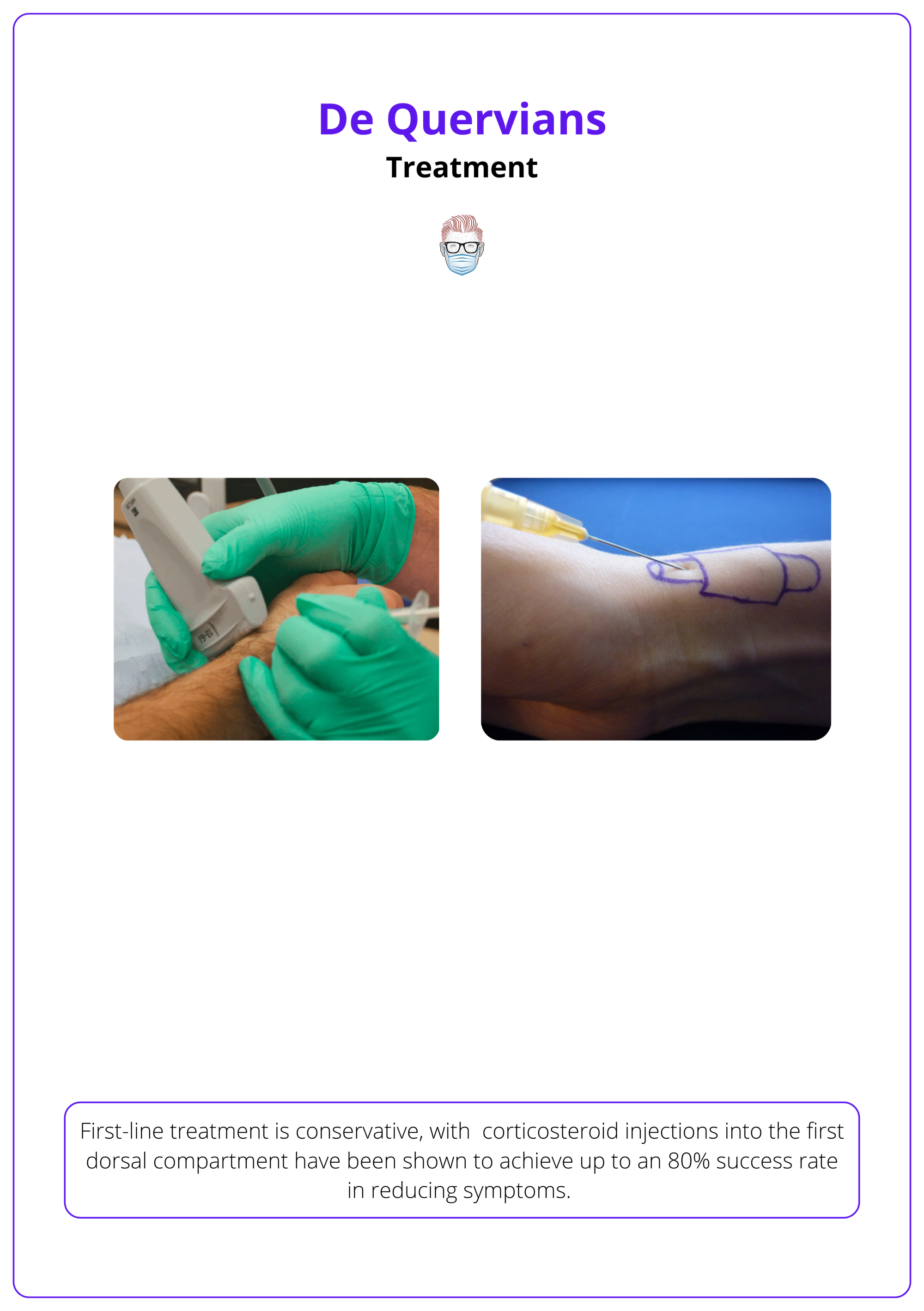
First-line treatment is conservative, with surgical intervention considered when conservative measures fail to relieve symptoms.
Non-Surgical Management
- Rest and avoidance of aggravating activities (especially repetitive thumb movements).
- Splinting (thumb spica splint) to immobilize and rest the affected tendons.
- Nonsteroidal anti-inflammatory drugs (NSAIDs) to manage inflammation and pain.
Steroid Injections
Corticosteroid injection into the first dorsal compartment (shown to have up to 80% success rate in reducing symptoms, though recurrence is possible if activity modifications are not made).
Surgical Treatment
Surgical release if conservative treatment fails after 2-3 months or if persistent symptoms significantly impact function. The procedure overview is as follows:
- Incision: The use of a zigzag or longitudinal incision
- Dissection: protect the superficial radial nerve branches.
- Release: Release of the fibro-osseous roof of the compartment to decompress APL and EPB tendons. Septation between APL and EPB must be carefully released to avoid incomplete decompression.
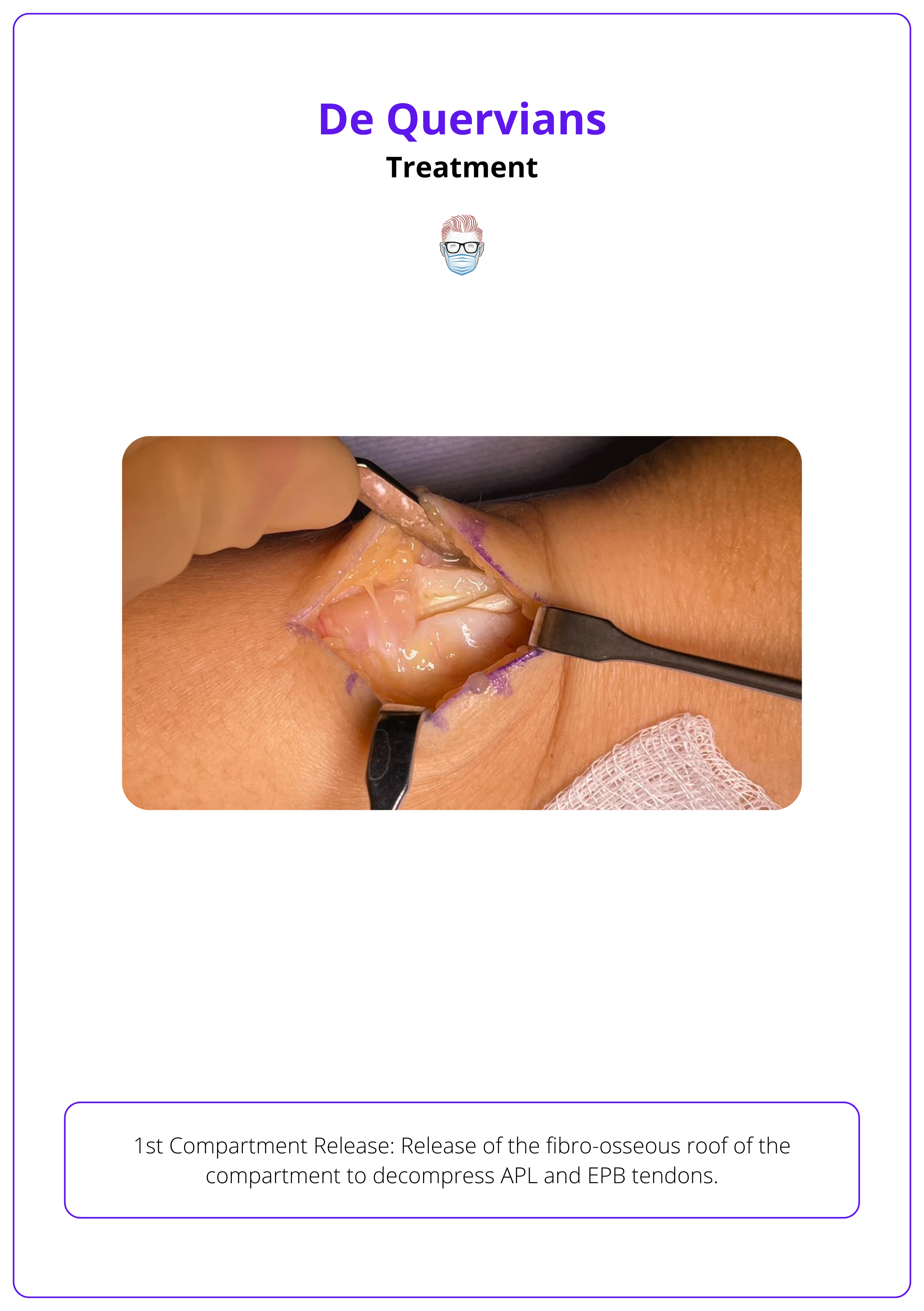
In cases where a septum divides the APL and EPB, the surgeon must release both compartments to ensure complete pain relief.
A septum is often present between the APL and EPB tendons in the first dorsal compartment, reducing the space and impacting both operative and non-operative management.
Complications
- Injury to the Superficial Radial Nerve: Can result in neuroma and persistent pain. Managing scar sensitivity and preventing neuroma formation are crucial.
- Entrapment of the APL or EPB: Incomplete release may lead to persistent symptoms.
- Tendon Subluxation: Can occur if the retinaculum is excessively released. Proper post-operative monitoring and rehabilitation are needed to prevent this.
Intraoperative identification of superficial radial nerve branches is critical to avoid neuroma formation, which can result in chronic pain
Conclusion
1. Overview of De Quervain's Disease: Explained de Quervain's disease as a form of stenosing tenosynovitis affecting the first dorsal compartment of the wrist.
2. Risk Factors and Epidemiology: Highlighted pregnancy and manual labor as significant risk factors, with an increased prevalence observed in new mothers due to repetitive lifting motions.
3. Pathophysiology and Etiology: Discussed the underlying causes of de Quervain's, focusing on the thickening and myxoid degeneration of the tendon sheaths.
4. Clinical Presentation and Diagnosis: Detailed the typical presentation with diagnosis primarily based on clinical findings and confirmed through provocative tests like Finkelstein's test.
5. Treatment Approaches: Outlined conservative treatments as the first line, with surgical intervention recommended for cases resistant to non-operative measures.
6. Potential Complications: Noted possible complications from surgical treatment, such as injury to the superficial radial nerve and tendon subluxation.
Further Reading
- Satteson E, Tannan SC. De Quervain Tenosynovitis. [Updated 2023 Nov 22]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK442005/
- Suwannaphisit S, Chuaychoosakoon C. Effectiveness of surgical interventions for treating de Quervain's disease: A systematic review and meta-analysis. Ann Med Surg (Lond). 2022 Apr 13;77:103620. doi: 10.1016/j.amsu.2022.103620. PMID: 35638053; PMCID: PMC9142670.
- Shuaib W, Mohiuddin Z, Swain FR, Khosa F. Differentiating common causes of radial wrist pain. JAAPA. 2014 Sep;27(9):34-6. doi: 10.1097/01.JAA.0000451875.71319.17. PMID: 25148441.
- Ilyas AM, Ast M, Schaffer AA, Thoder J. De quervain tenosynovitis of the wrist. J Am Acad Orthop Surg. 2007 Dec;15(12):757-64. doi: 10.5435/00124635-200712000-00009. Erratum in: J Am Acad Orthop Surg. 2008 Feb;16(2):35A. Ilyas, Asif [corrected to Ilyas, Asif M]. PMID: 18063716.
